HPV Vaccines and Cancer Prevention: How Far Have We Come?
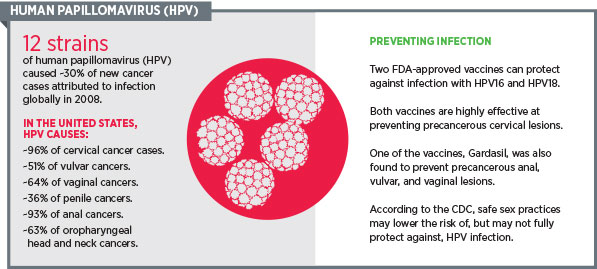
A world free of cervical cancer may not just be a dream, but may become a reality. Gardasil and Cervarix, two Food and Drug Administration-approved human papillomavirus (HPV) vaccines, are proving to be very effective in preventing infections with HPV subtypes 16 and 18, which cause the majority of cervical cancers. Gardasil also prevents infection with HPV subtypes 6 and 11, which cause genital warts.
A nine-valent vaccine, being developed by Merck and currently under investigation, covers HPV subtypes 31, 33, 45, 52, and 58, besides 6, 11, 16 and 18. This vaccine is currently under review by the FDA. But how effective is the nine-valent vaccine, and how is it better than Gardasil and Cervarix, which can prevent infection with the HPV subtypes that cause 70 percent of all cervical cancers?
In 2011, the International Agency for Cancer Research (IARC) expanded its list of carcinogenic HPV subtypes beyond HPV 16 and 18 to include HPV 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59. While HPV subtypes 16 and 18 are well-established as causative agents of cervical intraepithelial neoplasia (CIN), the precursors for invasive cervical cancers, HPV subtypes 31, 33, 35, 45, 52, and 58 are the next most frequent types detected in this disease, according to a 2012 publication by IARC.
A study published last week in Cancer Epidemiology, Biomarkers & Prevention looked at the types of HPV infections in 12,514 women, ages 15 to 45, enrolled in the placebo arms of three clinical trials testing the quadrivalent HPV vaccine. The study found that about 55 percent of CIN 1, about 78 percent of CIN 2, about 91 percent of CIN 3, and nearly 100 percent of adenocarcinoma in-situ lesions were attributed to seven of the nine HPV subtypes covered by the new investigational nine-valent HPV vaccine.
A closer look at the data showed that about 25 to 50 percent of the cervical precancers in these women harbored at least one of the HPV subtypes 31, 33, 45, 52, and 58, suggesting that the addition of these five subtypes to an HPV 16/18 vaccine could prevent almost 90 percent of invasive cervical cancer cases worldwide.
While more potent and effective vaccines promise near elimination of cervical cancer, a lack of public awareness and adherence to vaccination programs is hindering progress in the prevention of HPV-related cancers. According to a Centers for Disease Control and Prevention (CDC) report, vaccination coverage in the United States is increasing rather slowly among girls ages 13 to 17, a key group for whom vaccination is recommended. In 2013, 57.3 percent of girls in this age group had received at least one dose of HPV vaccine – up less than 4 percent from 2012, when the vaccination rate was 53.8 percent. Only 33 percent of girls had received the recommended three doses. In some states, this number was as low as 12 percent.
It appears that cervical cancer is not the only cancer that could be prevented by these vaccines. A significant proportion of vulvar, vaginal, penile, anal, oral, and other head and neck cancers are related to HPV infections. While wo do not yet have definitive evidence of protection against these cancers with HPV vaccines, it does seem like a possibility.
Bob Margolis, a three-time survivor of cancer, vouches for the importance of HPV vaccination in the AACR Cancer Progress Report 2014. Margolis, a sports writer and a father of three, shares his experience with a diagnosis of HPV-related stage IV head and neck cancer, and his commitment to encouraging people to talk about it and get help.
“It can be difficult to discuss getting a sexually transmitted cancer, but it is time to talk about it,” Margolis said. “We can prevent a generation of young Americans from having to go through the same experience I did.”
Learn more about Margolis’ journey and the cause he fights for in this video:
Besides vaccinating girls, the CDC recommends HPV vaccination for all boys, ages 11 or 12; for those through age 21, who have not already received all three doses; for gay and bisexual men; and for men with compromised immune systems.
Fortunately, there seems to be an increase in vaccination rate among teenage boys, from 20.8 percent in 2012 to 34.6 percent in 2013, according to the CDC. This is certainly a step in the right direction, but clearly, a lot more needs to be done if we are to exploit the true potential of vaccination and reap the benefits of one of the best tools we have so far in our efforts to prevent cancer.