Risk or Relief? Menopausal Hormone Therapy for Women With BRCA Mutations
Just last month, the U.S. Food and Drug Administration (FDA) removed the longstanding boxed warnings of increased cancer risk from several menopause hormone therapy (MHT) drugs. The original research from the Women’s Health Initiative (WHI) that precipitated the warnings, according to the FDA statement, had overstated the risks that MHT pose to many women, including the purported risks of developing invasive breast cancer. The decision to remove the warnings brought to the fore a decades-old scientific debate: Is MHT safe? Or do its purported cancer risks outweigh the benefits?
Aging Unexpectedly: The Challenges of Early Menopause in At-risk Women
This question is particularly acute for the subset of women living with pathogenic mutations in the BRCA1 or BRCA2 genes. Women who inherit these mutations face such a significant risk of developing ovarian and/or fallopian tube cancers that they often have the ovaries and fallopian tubes removed in a procedure known as bilateral salpingo-oophorectomy, which can reduce mortality by as much as 68%.
Oophorectomy, however, does carry a large drawback: a near guarantee of menopause shortly after the procedure. When oophorectomy is recommended in patients in their 30s or 40s, the procedure can cause menopause decades earlier than it would otherwise occur (the average age of menopause onset in the United States is 52).
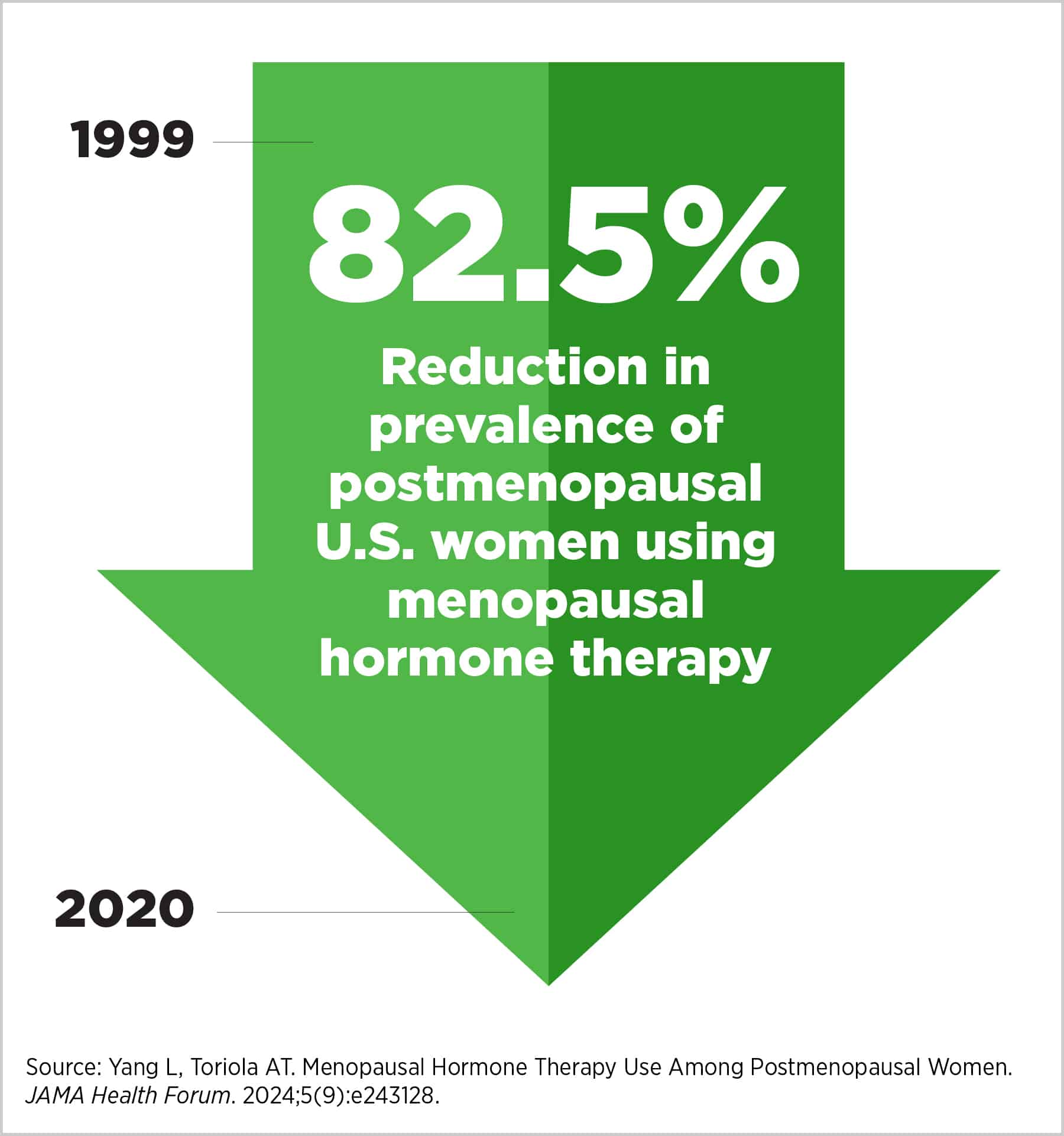
Because of lack of clarity around MHT’s safety, women with BRCA1 and/or BRCA2 mutations face an unpleasant choice following oophorectomy: an elevated risk of cancer if they take MHT, or early-onset menopause if they don’t. That general lack of confidence can be seen in the steep decline of MHT prescriptions in the United States since the institution of the boxed warnings in the early 2000s. From 1999 to 2020, the percentage of postmenopausal women with an MHT prescription plummeted from 26.9% to 4.7%—an 82.5% decrease.
“We cannot simply recommend a drastic surgery like oophorectomy for young women without offering a way for them to manage the well-established short- and long-term outcomes of surgical menopause,” Joanne Kotsopoulos, PhD—a scientist at the Women’s College Hospital Research and Innovation Institute in Toronto, Canada—who conducted a study to determine whether MHT use was associated with an increased risk in breast cancer for women with pathogenic variants of BRCA1 and/or BRCA2, said in a press release. “I believe we should educate patients and their health care providers on how we can safely balance the risks and benefits of MHT use to ensure longevity and improve quality of life.”
Clarity Amid Uncertainty: MHT and Breast Cancer Risk for Patients With BRCA1/2 Mutations
Hormone replacement therapy for menopause can provide much-needed relief for menopause’s often-unpleasant symptoms, including hot flashes, sleep difficulties, sexual dysfunction, psychological changes, and other problems. In any one of a variety of formulations that deliver exogenous hormone combinations, MHT manages the symptoms by reopening the hormonal tap that menopause shuts off.
However, scientists have known for many decades that breast cancers often rely on female hormones, such as estrogen, to develop and proliferate. For instance, a key element in determining which drugs can or should be used to treat breast cancer is whether the breast cancer cells express hormone receptors.
Breast cancers that test positive for hormone receptors, or HR-positive breast cancers, account for nearly 80% of all breast cancer cases. The age at which women first become pregnant—a known breast cancer risk modifier, with later ages being associated with increased risk—demonstrates how exposure levels to certain sex hormones can influence women’s health.
To clarify the safety of MHT for women with pathogenic BRCA1 and/or BRCA2 mutations (mutations that can also increase breast cancer risk), Kotsopoulos and her colleagues conducted a matched prospective analysis. They presented their results at the 2025 San Antonio Breast Cancer Symposium (SABCS).

The researchers created 676 matched pairs of menopausal women who either did or didn’t take MHT. Pairs were formed to measure multiple variables that could impact patients’ breast cancer risk, including whether they had BRCA mutations, how old they were when they began menopause, and which MHT formulations they used. Though participants’ ages ranged from 22 to 76, the study population skewed younger due to the participation of women who underwent early oophorectomy, with an average age of 43.8. Women in the study took either estrogen alone, progesterone alone, estrogen and progesterone, tibolone, or conjugated estrogen and bazedoxifene.
The follow-up clock, so to speak, started when the MHT-exposed patient in the matched pair began taking MHT. After an average follow-up time of 5.6 years, menopausal women who took MHT did not face any significant increases in breast cancer incidence when compared to their menopausal counterparts who did not take MHT, although Kotsopoulos noted that this result may change with longer follow-up. When patients with pathogenic BRCA1 and BRCA2 mutations were compared with their wild-type-BRCA counterparts, the effect held: MHT use didn’t increase breast cancer risk.
In fact, Kotsopoulos’ study showed that, for some formulations of MHT, the association with breast cancer incidence was outright negative. Using estrogen-only MHT was associated with a 63% reduction in breast cancer risk. And although only 43 women in the study used the MHT formulation of conjugated estrogen and bazedoxifene, no breast cancer cases were observed in any of those 43 women.
Everybody’s risk tolerance is different, and no drug is a panacea, but for women with BRCA mutations who face the difficulties of menopause after oophorectomy, our results suggest MHT is safe and can improve what might otherwise be a ‘rock and a hard place’ situation.
For her part, Kotsopoulos is optimistic about MHT’s safety in women with inherited mutations in BRCA1 and BCRA2, and she pointed to the need for future research to clarify possible protective effects. “Hypothetically, conjugated estrogen and bazedoxifene could be used to mitigate breast cancer risk by avoiding progesterone, which is thought to be the breast cancer risk-associated component of MHT. Future trials will be necessary to test this hypothesis,” she said.
It is important to note, however, that the patient population in Kotsopoulos’ study may skew younger than the general population’s cohort. Follow-up was a limiting factor as well, given that breast cancer incidence may increase with time.
Even so, Kotsopoulos considers her study to be not just good news but well-timed good news. “Between our results and the FDA’s easing perception on MHT’s safety profile, I think we may see more women electing to live their lives with less worry and fewer symptoms,” she said. “Everybody’s risk tolerance is different, and no drug is a panacea, but for women with BRCA mutations who face the difficulties of menopause after oophorectomy, our results suggest MHT is safe and can improve what might otherwise be a ‘rock and a hard place’ situation.”
Balancing Act: What Experts Think About MHT and Breast Cancer
In a SABCS 2025 panel, clinicians from around the world addressed the timely question of how researchers and practitioners should think about MHT and breast cancer in the context of a shifting consensus on risk. Moderated by Tara Sanft, MD, an associate professor of medicine and director of the Survivorship Program at Yale Cancer Center, the session “Balancing Act—Hormone Replacement Therapy in Breast Cancer Care” surveyed the landscape of MHT use.

The session highlighted just how divided clinical opinion remained. Of clinicians polled in the room during the session, the majority of them said they were uncomfortable prescribing systemic MHT to breast cancer survivors, and about half of them said they would be supportive of others prescribing it to some survivors.
Patient advocate, Thelma Brown—a two-time breast cancer survivor who experienced early menopause at age 39 after oophorectomy—articulated the sense of confusion that patients may face in such an environment. “Patients are not asking for guarantees: They’re asking for clear guidance based on the evidence,” she said. “Survival matters, and so does living well. Quality of life is not optional—it is core to healing.”
Presenter Lisa Larkin, MD, a longtime women’s health internist, emphasized the need for context above all, noting that randomized clinical trials can provide more answers. With the FDA’s warning removed, Larkin highlighted the centrality of the individual patient in each case, with emphasis on the difference between absolute risks and relative risks.
She pointed to the risks that untreated early menopause can itself cause, including issues with bone and brain health. “The data are overwhelmingly clear: there are significant health consequences of early menopause,” she said.
For those who have registered for the symposium, sessions may be viewed on the SABCS virtual platform through March 31, 2026.