Geographic Disparities in Progress Against Lung Cancer
A recent study showed declines in lung cancer death rates among U.S. women have lagged in two geographic hot spots.
Lung cancer is the leading cause of death from cancer among women in the United States, with more than 70,000 deaths from the disease projected to occur in 2018 alone, according to
analysis of data from the Centers for Disease Control and Prevention’s National Center for Health Statistics.
Despite these grim statistics, we have been making progress against lung cancer for women, as illustrated by the fact that the overall lung cancer death rate among all U.S. women – meaning the number of deaths per 100,000 women in the United States per year – has been falling steadily since the mid-2000s.
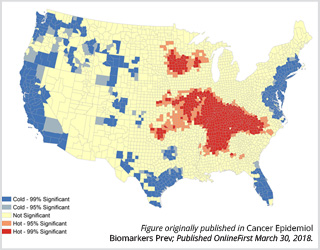
But those declines in lung cancer death rates among women in one region covering central Appalachia and southern parts of the Midwest, and another covering northern parts of the Midwest have lagged, according to a new study, published recently in Cancer Epidemiology, Biomarkers & Prevention, a journal of the American Association for Cancer Research.
More specifically, the study showed that from 1990-1999 to 2006-2015, lung cancer death rates among women rose by 13 percent in a hot spot encompassing 669 counties in 21 states in central Appalachia and southern parts of the Midwest. During the same period, in a second hot spot that encompasses 81 counties in four states in the northern Midwest, lung cancer death rates among women rose by 7 percent. In the remainder of the contiguous United States, lung cancer death rates among women fell by 6 percent.
The research team, which was led by Katherine Ross, MPH, also compared lung cancer death rates among women in each hot spot with those among women in the remainder of the United States. In 1990, the death rate for the largest hot spot was 4 percent lower than the death rate for non-hot spot regions, but in 2015, it was 28 percent higher. For the second hot spot, the death rate was 18 percent lower than the non-hot spot death rate in 1990 but equivalent to the non-hot spot death rate in 2015.
Tobacco smoking causes about 80 percent of the lung cancer cases diagnosed in U.S. women, according to the National Cancer Institute (NCI).

“We wanted to see if there were geographic differences in this decline [the lung cancer death rate decline] so that we could identify places in the United States where women might benefit from targeted tobacco control and smoking cessation programs, and other interventions aimed at reducing the burden of lung cancer,” said Ms. Ross, who is a graduate student in the Department of Epidemiology of the Rollins School of Public Health at Emory University, Atlanta.
“We know that Midwestern and Appalachian states have the highest prevalence of smoking among women and the lowest percent declines in smoking in recent years, so it is perhaps not surprising that we found that women in these areas experienced a disparity in lung cancer death rates,” she continued. “This geographic disparity may widen unless we specifically aim to reduce tobacco use among women in these hot spots.
“There are several effective tobacco control policies available, such as increased excise taxes on tobacco and comprehensive smoke-free air laws that ban smoking in the workplace, restaurants, and bars,” Ms. Ross noted. “However, many states in our identified hot spots either do not have these measures in place, or they are comparatively weak and could be strengthened.”
To conduct the study, Ms. Ross and her colleagues used data on the number of lung cancer deaths among women obtained from the NCI’s Surveillance, Epidemiology and End Results Program (SEER) database to calculate age-standardized lung cancer death rates for each county in the contiguous United States from 1990 to 1999 and from 2006 to 2015. They then calculated the absolute change and the relative change in the death rates between the two periods for each county.
The researchers used a software tool called ArcGIS to identify clusters of counties with increases or small decreases in lung cancer death rates between the two periods, called hot spots.
According to Ms. Ross, the main limitation of the study is that the researchers are not able to draw any conclusions about whether or not differences in tobacco control are responsible for the trends they observed. “In addition, in some counties there was not enough information about rates available to draw conclusions about their trends in lung cancer mortality among women, which means that the results of the study might not apply to those counties,” Ms. Ross added.