
Exciting Precision Medicine Possibilities for Liquid Biopsy
Guest Post by Wafik S. El-Deiry, MD, PhD, FACP
Fox Chase Cancer Center
The idea of a less invasive way to get accurate information about a cancer from a blood sample, also known as liquid biopsy, is gaining much popularity because technology is finally catching up with this vision. Good examples of how this technology is already being applied were recently highlighted in The New York Times (examples here and here); Newsweek; the Philadelphia Inquirer; and at the AACR Annual Meeting 2015 (read more here and here).
What are liquid biopsies?
For several years we have been able to count circulating tumor cells (CTCs) from a tube of blood from patients with advanced prostate cancer, breast cancer, or colorectal cancer. Why do we do this and how does it help? It has been shown that the number of CTCs in a blood sample correlates with overall patient survival in these diseases, i.e., it is a prognostic marker. In current practice, it is possible to count CTCs by using a U.S. Food and Drug Administration-approved test known as the CellSearch test. Blood tests such as PSA or CEA have been used to diagnose certain cancers, but the markers these tests measure are not always elevated, even in the case of metastatic disease. Therefore, measuring CTCs provides a marker that can be followed while patients are receiving therapy or as a means to detect relapse of disease. The tests are non-invasive, carry minimal risk, and are less expensive than scans that expose patients to low amounts of radiation that can add up.
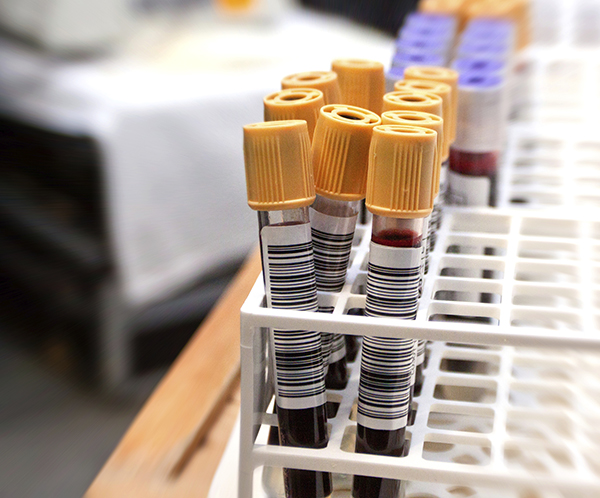
The idea of liquid biopsy for cancer diagnosis and treatment is gaining in popularity.
With hundreds of genetic drivers that could be targeted by therapeutics, it is important to verify the presence of the target in the tumor, to assess the tumor’s response to the targeted therapy including signaling and evidence of tumor cell death, and to detect resistance mechanisms. One path forward involves use of liquid biopsy to exploit the power of this latest technology to personalize therapy. In this regard, recent papers published in Cell and Nature Medicine are steps in the right direction as far as dynamic interrogation of tumor cells for drug sensitivity and monitoring response to therapy.
What we know
Analysis of circulating DNA or other blood components is currently a hot area for investigation. Liquid biopsy technologies are proliferating and include tests to measure circulating DNA and exosomes, chemotherapy drug level tests, and various tests of immune cells or cytokines. Some of the tests can provide information that previously could only be obtained from a tumor biopsy or from a tumor specimen removed at the time of surgery. Thus, with a non-invasive test, it is now possible to determine that a colorectal cancer has a KRAS driver mutation that predicts resistance to targeted therapy by cetuximab or panitumumab. It is also possible to quantify the levels and monitor the levels of the mutant DNA as the patient receives therapy.
There is heterogeneity among patients, and it has been shown that tumor cells recovered from blood can grow and be tested in culture or after implantation in mice against various therapeutic agents. The ability to interrogate the genomics or drug sensitivity provides a way to direct therapy for individual patients (see Gallant et al., 2013 and Yu et al., 2014). New devices are being developed including one that uses sound waves to get the tumor cells diverted in a flow channel away from the white blood cells. This is important to obtain a pure population of tumor cells for genomic analysis or drug sensitivity testing, and is promising because sound waves do not perturb the tumor cells and provide high quality living cells for further analysis.
What’s next
One of the exciting directions for the field involves routine single-cell genomic analysis of circulating tumor cells. This will inform about the heterogeneity of a patient’s tumor and how different patients’ tumors compare to each other, as well as provide information on prognosis, drug sensitivity, and resistance potential. Of course, if breakthroughs are made that make it possible to culture CTCs more easily, this could also be very helpful for drug testing.
There is much progress in these areas at Fox Chase Cancer Center that is preclinical, and some data from correlative studies in the clinic that hold promise – for example, we are learning how to use liquid biopsy to determine how to best use immune checkpoint therapies. We are also exploring how to optimize chemotherapy dosing through blood tests that monitor metabolism in a specific patient. In the future, monitoring the activity of drug metabolizing genes and markers of higher or lower drug metabolism should allow more tailored dosing of chemotherapy.
We isolated circulating tumor cells in cerebrospinal fluid (CSFTCs) and identified some vulnerabilities that are relevant for therapy of patients with breast cancer and brain metastases. This work suggested that COX2 may be worth targeting in combination therapy in patients with breast cancer and brain metastases.
We need to embrace the challenge of using information we can derive from circulating DNA, CTCs, or other blood components to better monitor and treat patients. Clearly other components of blood hold promise, including exosomes, micro-RNA, metabolomics, as well as immune system analysis.
The impact of liquid biopsy on precision medicine remains in its infancy with many exciting future directions. Clearly the future will involve more sophistication in what is detected and what can be done with the information. We must go beyond what we know now in measuring driver genes, or actionable targets. We need to go further in detecting drug resistance mechanisms and have a plan of action for adjusting therapy for specific patients. Technology must evolve to allow more facile discovery of resistance mechanisms from blood samples as this could make the tests even more helpful in the clinic. The ease with which the tests can be done with minimal risk and not too much expense bodes well for the ability to personalize therapy for a diverse population with heterogeneous tumors.

Dr. El-Deiry. Photo courtesy of Fox Chase Cancer Center.
Wafik S. El-Deiry, MD, PhD, FACP, was appointed deputy cancer center director for translational research and co-program leader in molecular therapeutics at Fox Chase Cancer Center in 2014. With a focus on colorectal cancer and precision medicine, El-Deiry is an international leader in translational research and one of 40 active American Cancer Society Research Professors. He earned both his MD and PhD from University of Miami School of Medicine. After completing an internal medicine residency at Johns Hopkins Hospital in Baltimore, Maryland, El-Deiry completed an oncology fellowship at Johns Hopkins Oncology Center. Prior to joining Fox Chase, El-Deiry served as the Rose Dunlap Professor of Medicine, chief of the Hematology/Oncology Division, and associate director for translational research at Penn State University’s Milton S. Hershey Medical Center and the Penn State College of Medicine. He was an investigator of the Howard Hughes Medical Institute at the University of Pennsylvania where he served as a professor of medicine, pharmacology, and genetics, and co-leader of the Radiobiology & Imaging Program at the Abramson Cancer Center. El-Deiry has co-authored more than 300 peer-reviewed articles and edited five books. He has served in leadership positions on the editorial boards of the Journal of Clinical Investigation and Cancer Biology and Therapy, a publication he co-founded in 2001.
El-Deiry is known for discovering p21(WAF1) as a p53 target gene, universal cell cycle inhibitor, and tumor suppressor gene that for the first time explained the mammalian cell stress response – the most highly cited original work published in the journal Cell over the last 20 years. His laboratory unraveled cell death signaling pathways in the DNA damage response and screened for small molecule therapeutics that have been taken into clinical trials.
El-Deiry joined the American Association for Cancer Research in 1995. He currently serves on the editorial board of the AACR’s journal Cancer Research and previously served on the board of Clinical Cancer Research. He received the Jeannik M. Littlefield-AACR Grant in Metastatic Colon Cancer Research in 2006. El-Deiry has served as a member of the AACR’s Research Grant Review Committee as well as its Clinical Research and Experimental Therapeutics Awards Committee, and as a mentor at the fourth annual grant writing workshop for associate members in 2001. He organized an AACR Special Conference on Cell Death Mechanisms and Cancer Therapy in 2010. El-Deiry has been an active participant in many AACR Annual Meetings, serving as chair of the Cell Cycle and Cell Death Committees as well as chair of a number of mini-symposiums. At the AACR Annual Meeting 2012, his laboratory presented 22 abstracts, the third highest in the world at the time. El-Deiry also served on the AACR Science Policy and Legislative Affairs Committee from 2005-2008.


Yeah, we noticed that too. QIAGEN method is losing too much…1 or 2 mL of plasma is not enough for cell-free DNA recovery. We experienced 30-40% failure in NGS library prep!! I’d live to learn more about CirculoGene!
Circulating cell-free DNA could be new generation of liquid biopsy for cancer management. However, limitations like large volume of input, low recovery efficiency, labor intensiveness, and difficult for automation had hindered its clinical applications. Now, people are talking about last-generation of cfDNA-based liquid biopsy using a finger-tip volume of blood for tumor monitoring. Check it out at 2015 ASCO abstract by CirculoGene Diagnostics!!