From Treatment to Prevention: How Vaccines Are Reshaping the Fight Against Pancreatic Cancer
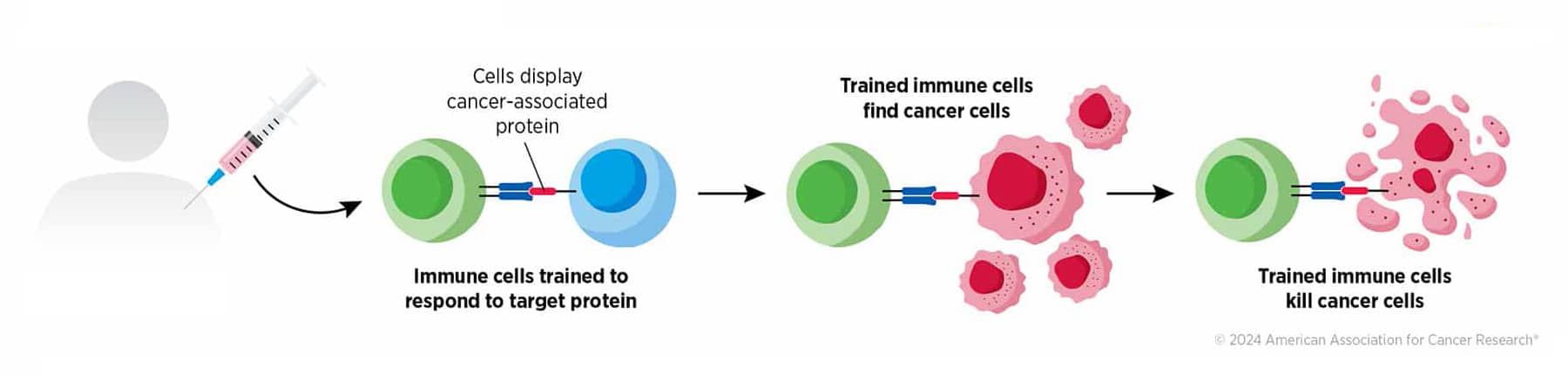
As one of the milestones of modern medicine, vaccination has been very effective at reducing the spread of infectious diseases. Drawing from this experience, researchers have been investigating ways to use vaccines as a form of immunotherapy to prevent and treat cancer by training the immune system to recognize and attack cancer cells. Read these previous posts for an introduction to cancer vaccines and some of the latest experimental strategies from the field.
Cancer vaccines have evolved in parallel with the wider field of cancer immunotherapy and, after leaps forward and setbacks, have now reached what the researchers consider an inflection point: Thanks to the convergence of enabling scientific advances—including new vaccine delivery strategies and the ability to identify cancer-specific antigens, a deep molecular understanding of the inner workings of the immune system, and other immunotherapy breakthroughs that led to the discovery of immune checkpoint inhibitors—the last decade has been transformative for cancer vaccines, particularly for certain challenging cancer indications, such as pancreatic cancer.
The case of cancer vaccines for pancreatic cancer is especially relevant because this disease is still one of the most challenging cancers to treat and has long been considered immunologically “cold,” or capable of going unnoticed by the immune system. In fact, pancreatic cancer is characterized by a highly immunosuppressive microenvironment, low expression of immunogenic cancer-specific antigens, and defects in the antigen presentation mechanisms, so that T cells have a hard time “seeing” and infiltrating the tumor. Because of these features, pancreatic cancer is highly resistant to immune checkpoint inhibitors. However, researchers have discovered strategies to circumvent the lack of immune recognition and help turn pancreatic cancer into a vaccine-responding disease.
Cancer Research Catalyst had a conversation with cancer vaccine expert Elizabeth M. Jaffee, MD, FAACR, a former AACR President and an editor-in-chief of the AACR journal Cancer Immunology Research, to review the current landscape of pancreatic cancer vaccines, including the latest breakthroughs, the clinical progress, and the path toward new effective vaccine-based strategies.
Jaffee, who is the deputy director of the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University School of Medicine, is an international leader in cancer immunology. Her pioneering work led to the development of one of the first pancreatic cancer vaccine approaches and helped advance the concept of harnessing the immune system to fight cancer.
“Any cancer can be recognized by the immune system if you deliver the right antigens in the right context,” said Jaffee emphasizing the potential of cancer vaccines.
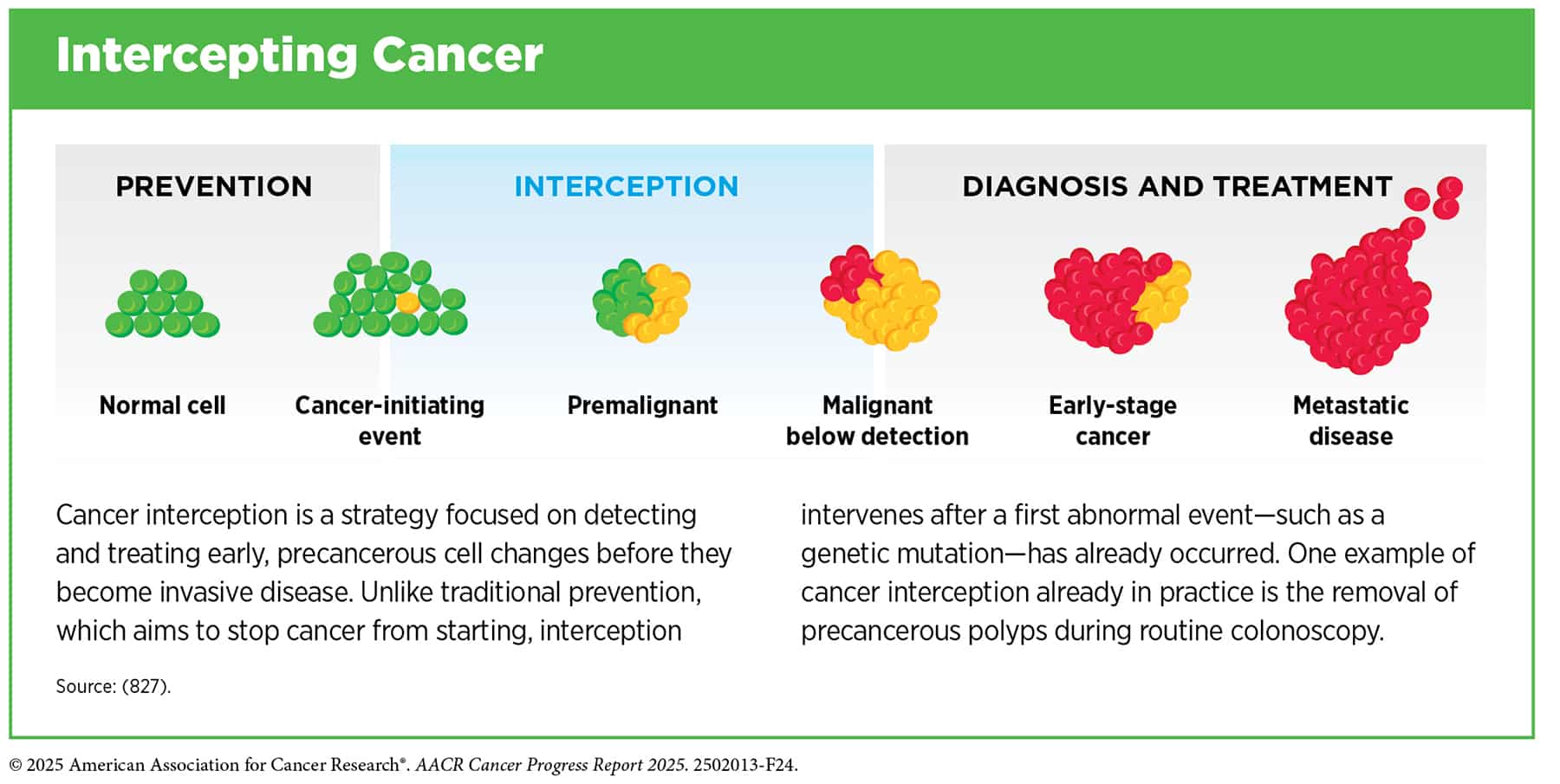
Continuing on her trailblazing path, Jaffee and collaborators recently explored the use of a vaccine to prevent pancreatic cancer development in individuals at high risk, expanding the scope of vaccines from cancer therapy to interception.
Harnessing Neoantigens to Expand Immune Recognition of Pancreatic Cancer
The new generation of vaccines for pancreatic cancer is driven by precision medicine approaches and leverages newer delivery technologies to induce immune responses against proteins that are specifically expressed by cancer cells, called neoantigens. Since neoantigens are produced as a result of mutations, they can be recognized by the immune system as foreign and trigger a strong response, making them highly specific targets for immunotherapy.

Jaffee’s team is pursuing an off-the-shelf approach for neoantigen-based vaccination by targeting six common KRAS driver mutations, which are present in up to 90% of pancreatic ductal adenocarcinomas (PDACs). “We are targeting the neoantigen that we know is the reason why pancreatic cancer develops,” Jaffee said. The vaccine, called mKRAS-VAX, is delivered as a pool of synthetic peptides.
This strategy was applied with therapeutic intent to stop pancreatic cancer from coming back after surgical resection. At this stage, when the disease burden is minimal and the immune system is still relatively fit, it is easier to induce a good immune response, observed Jaffee.
In a recent study, the mKRAS-VAX vaccine was given with the checkpoint inhibitors nivolumab (Opdivo) and ipilimumab (Yervoy) as adjuvant therapy to 12 patients with KRAS-mutant pancreatic cancer after standard-of-care surgery, chemotherapy, and radiation. The researchers observed a significant increase in vaccine-generated T-cell responses in 91.7% of patients, and high T-cell responses correlated with longer disease-free survival. After a median follow up of 35.8 months, 4 out of 12 patients remained disease-free and received booster doses of the vaccine every three months for an extended treatment phase. In these patients, mutant KRAS-specific T-cell responses persisted for the remainder of the study period.
A New Frontier for Cancer Vaccines: Disease Interception
So far, most of the studies on cancer vaccines have focused on the therapeutic setting, aiming to prevent disease recurrence. Jaffee and collaborators believe that another ambitious goal should be to use vaccines to intercept cancer in individuals at risk.
Since PDAC evolves over time from precursor lesions that are driven by KRAS mutations, the researchers saw a potential window of opportunity to prevent cancer development in high-risk individuals with hereditary predisposition to PDAC by vaccinating against mutant KRAS.
“With early-onset cancers on the rise, wouldn’t it be amazing if we had vaccines that could prevent cancer in young people who are at risk but are not eligible for screening yet and often end up being diagnosed with metastatic disease?” noted Jaffee.
The latest work from the team, which was just published in the AACR journal Cancer Discovery, puts us a step closer to the goal. In a first-in-human study, the researchers gave the mKRAS-VAX vaccine to 20 individuals with family history of pancreatic cancer or with a genetic predisposition for the disease and with small precancerous lesions, typically cysts, on their pancreas.
Results showed that vaccination was safe and well tolerated and, importantly, it elicited mutant KRAS-specific T-cell responses in 18 participants, corresponding to 90% of the study population. These responses persisted for up to two years. Furthermore, at a median follow-up of 16.5 months, none of the study participants had developed PDAC, and 37.5% of the cohort experienced cyst reduction or resolution, while in a similar group of unvaccinated individuals that rate was 6.8%. “We are very excited about these results,” said Jaffee.
A Personalized Vaccine Strategy
An alternative approach for neoantigen vaccination is to custom-make the vaccine for each individual patient based on specific mutations identified by sequencing that patient’s tumors.
Although the overall mutation burden in pancreatic cancer is modest, research has indicated that a few high-quality patient-specific neoantigens might correlate with immune response and patient survival and that these neoantigens can be sequenced and encoded into a personalize vaccine. The idea is to help the immune system focus on the most promising angles from which to attack the cancer.
For this strategy, the researchers used mRNA as a delivery platform. mRNA-based vaccines are easy to make and deliver and have demonstrated a favorable safety profile across multiple clinical studies and real-world use.

Long-term follow-up results from a phase I trial of the personalized mRNA vaccine autogene cevumeran were discussed at the AACR Annual Meeting 2026. The vaccine was given to 16 patients with resected PDAC in combination with the anti‑PD‑L1 therapy atezolizumab (Tecentriq) and chemotherapy. Initial results had showed vaccine-induced neoantigen‑specific T‑cell responses in eight patients and longer recurrence‑free survival in responders than in nonresponders. After a median follow-up of 4.2 years, vaccine-induced T cells persisted, and responders still had significantly prolonged survival compared to nonresponders. Four to six years after surgery, 7 of the 8 vaccine responders were alive, while only two of the nonresponders were alive during the same time period.
Further studies of the patients’ immune responses will help better understand how the personalized neoantigen mRNA vaccine is interacting with the immune system, Jaffee suggested. For example, she noted, even though the vaccine encoded up to 20 neoantigens per patient, responders only had T-cell responses against a few of those neoantigens. “We need to better understand why some antigens trigger a response and some don’t. Are some of the neoantigens not important, or are they just not being effectively presented to the immune system?”
Building on Encouraging Early Clinical Results
The early indications of correlation between immune responses to the vaccines and long-term survival have sparked enthusiasm.
“Our field is nascent, it is early, but I am cautiously optimistic: We are seeing some successes that we never saw before for pancreatic cancer,” noted Jaffee. “Even though these are small phase I studies that were not designed to assess clinical outcomes, they have been useful in providing proof of concept that has led us to push forward in larger studies to determine the true value of these vaccines.”
We are seeing some successes that we never saw before for pancreatic cancer.
She added that researchers in the field are eagerly awaiting the findings of ongoing phase II studies that will show whether the initial promising results will hold up in larger populations.
A phase II randomized study is currently underway to evaluate the safety and efficacy of autogene cevumeran combined with standard-of-care chemotherapy and with immunotherapy in comparison with standard-of-care in patients with resected PDAC who have no evidence of disease after surgery.
Jaffee noted that mKRAS-VAX is not in phase II studies. However, a phase II trial is assessing another peptide KRAS vaccine that delivers mutant KRAS to the lymph nodes, and she expects the results will be informative.
Lessons From Long-term Pancreatic Cancer Survivors of a First-generation Vaccine
In the era before neoantigen-based vaccines, Jaffee and team explored an earlier form of cancer vaccination through whole‑cell cancer vaccines. These use entire cancer cells as the antigen source, thus exposing the immune system to a broad collection of cancer antigens at once. Jaffee and colleagues pioneered this approach by developing GVAX, which uses irradiated pancreatic tumor cells that are genetically engineered to produce GM-CSF, a protein that attracts immune cells, to serve as an intrinsic booster to potentiate the T-cell response.
Although whole-cell vaccines are not easy to translate into a drug product on a large scale and newer and more efficient vaccine technologies are now available, they have been of great value as a tool to study the immune responses while giving small groups of patients an opportunity for longer-term survival, said Jaffee.
“I have what I call the ‘20-year club’ of quite a few patients with pancreatic cancer who were vaccinated [with GVAX] between 1997 and 2000. One patient just died in his 90s of noncancer-related causes. We have seen clinical activity, and that was before the advent of immune checkpoints,” Jaffee noted. “In these individuals there was no disease recurrence, so there was no cancer tissue to study. However, by analyzing their peripheral blood, we can find evidence of their immune response to the specific antigens expressed by the vaccine, characterize the type of T-cell responses, and track them over time.”
I have what I call the ‘20-year club’ of quite a few patients with pancreatic cancer who were vaccinated [with GVAX] between 1997 and 2000. One patient just died in his 90s of noncancer-related causes.
A National Concerted Effort to Push Cancer Vaccines Forward
In an effort to catalyze the momentum for the field of cancer vaccines, a public-private partnership spearheaded by National Cancer Institute director Anthony Letai, MD, PhD, FAACR, and led by the Foundation for the National Institutes of Health (FNIH) is set to raise nearly $200 million to fund clinical trials for cancer vaccines to prevent recurrence of hard-to-threat cancers. This initiative was discussed by Letai as one of NCI’s priorities at the AACR Annual Meeting 2026.
A roadmap for the clinical trials was devised by the Cancer Vaccine Advisory Committee, a nationwide panel of experts from academia, industry, and nonprofits, including AACR, cochaired by Jaffee.
The committee identified some of the emerging vaccine technologies that are ready to advance in clinical trials, with the plan to support three different studies. “We are discussing a comparison of mRNA versus long peptides or even a ‘prime-boost’ strategy with mRNA and peptides given sequentially to maximize both CD4-positive and CD8-positive T-cell responses,” explained Jaffee.
The experts are also discussing the type of approach (personalized or shared cancer neoantigens, or both) and what cancer types to include in the trials. The second step of this ambitious plan, Jaffee added, will be to improve the engineering of mRNA and peptide vaccines to induce the best range of T cells and to develop more assays to monitor the immune response.