
What Does It Mean to Be Diagnosed With Li-Fraumeni Syndrome?
Chenia Lloyd-Gascho was only 8 years old when he learned he was highly likely to get cancer at some point in his life—though, given his age, it would take a few years for that to truly resonate. At the time, he only knew he had “some cancer thing.” That “thing” is a rare hereditary condition known as Li-Fraumeni syndrome that dramatically increases the risk of developing cancer over the course of a person’s lifetime.

“It was pretty confusing, and I didn’t fully grasp what was happening at the time,” said Chenia, who shared his story in the AACR Pediatric Cancer Progress Report 2025. “I got pulled out of school every three months for scans and tests, but I didn’t fully understand why.”
Now 19, Chenia is well aware of what Li-Fraumeni syndrome is, of the routine monitoring—or surveillance—that children with this syndrome undergo to catch early signs of cancer, of the psychological toll it takes on someone so young, of what it feels like when those tests do find something, and what others diagnosed with Li-Fraumeni syndrome may be able to learn from his experience.
What Is Li-Fraumeni Syndrome?
Li-Fraumeni syndrome is named after National Cancer Institute researchers Joseph F. Fraumeni Jr., MD, FAACR, and Frederick P. Li, MD, FAACR, who first hypothesized about the possibility of a familial syndrome that could cause cancer in 1969—when little was known about the role genetics played in cancer’s development. By the late 1980s, they identified 24 families with well-documented cases of a hereditary syndrome that led to multiple types of cancer and published their results in the AACR journal Cancer Research. (Read this AACR Stories piece about Li and Fraumeni’s history-making work to define one of the first cancer predisposition syndromes.)
While they had identified this pattern of cancer passed down within families, they had not yet determined the cause. That discovery was made in the 1990s by David Malkin, MD, FAACR, along with Li, Fraumeni, and other colleagues who found that it was due to inherited—or germline—mutations in the TP53 gene.
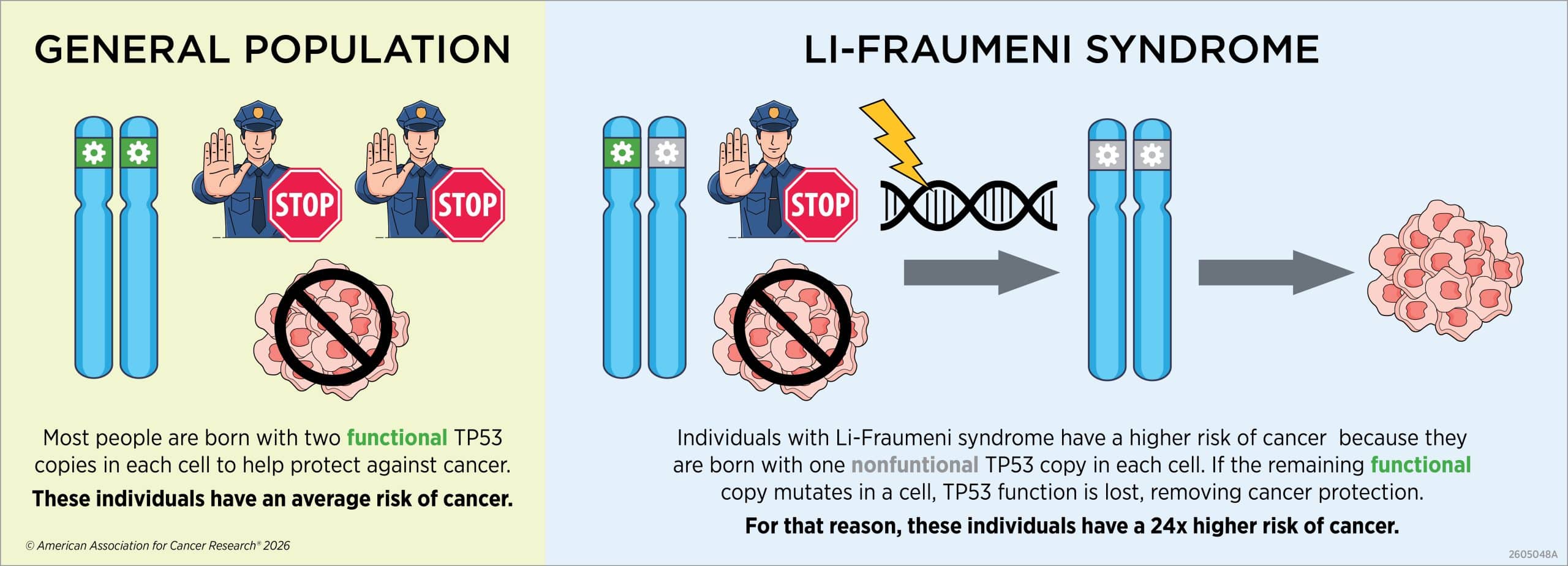
When functioning properly, TP53 acts as a tumor suppressor gene because it produces the p53 protein, which helps repair DNA damage in cells and can trigger cell death if the damage is irreparable. This process can prevent damaged cells from replicating and forming a tumor.
Almost every cell in a person’s body has two copies of TP53, but in people with Li-Fraumeni syndrome, one of those copies is mutated and cannot produce p53. However, as long as one TP53 gene in each cell is working, cancer is unlikely to develop. But if the functional TP53 gene in a single cell is lost over time (which is known as loss of heterozygosity) or altered (which is known as a somatic mutation), then cancer could develop in the body part where that cell is located.
While Li-Fraumeni syndrome is inherited in most cases, it can also form due to de novo mutations, meaning it is not passed down but occurs during a person’s development prior to birth. In these instances, TP53 may only be mutated in some cells in the body, which is called mosaic Li-Fraumeni syndrome.
Chenia said that none of this made sense until he was around 10 or 11 when his mom took him to the Li-Fraumeni Syndrome Association Conference where a doctor offered a more child-friendly analogy.
“He explained that normal people have two cops that stop cancer from forming, but for people who have Li-Fraumeni syndrome, there is one cop who is not able to do his job,” Chenia said. “That was when it finally clicked for me. And that was also when it finally landed that I had a very high chance of developing cancer.”
How Likely Are People With Li-Fraumeni Syndrome to Get Cancer?
Li-Fraumeni syndrome is a rare condition that is estimated to affect 1 in 3,000 to 1 in 20,000 individuals. People with this syndrome are 24 times more likely to get cancer in their lifetime compared with the general population. The chances of cancer in individuals with Li-Fraumeni syndrome are near 100% in females and around 70% in males. Additionally, over half of individuals with Li-Fraumeni syndrome are diagnosed with multiple types of cancer over the course of their lives with the average age of first cancer diagnosis being 33.7 for women and 45 for men.
In males, the most common first cancers are soft-tissue sarcomas and central nervous system tumors, such as glioma, choroid plexus carcinoma, and medulloblastoma, with a 20% lifetime cumulative incidence of these cancers. For females, breast cancer is most common and accounts for 57% of first cancers by age 60. Across both sexes, there is also a 20% to 40% chance of getting cancer before turning 20, with soft tissue and bone sarcomas, central nervous system tumors, and adrenocortical tumors being the most common. Less frequently, Li-Fraumeni syndrome has also been associated with prostate, lung, colorectal, ovarian, stomach, thyroid, skin, and blood cancers.
“Learning about my chances of getting cancer definitely changed how I viewed going about life,” Chenia said. “I started to question whether I had to make long-term healthy decisions.” He joked that as a 10-year-old that meant wanting to fill up on candy and ice cream. “I figured why not, since I don’t have to worry about heart attacks, which is a funny way to think about it looking back.”
But the real difficulty, Chenia explained, is the thought that cancer can come at any moment for you or your loved ones since it is a familial condition. Chenia lost both his aunt and grandmother to cancer. The latter particularly affected him because, at 12, he was old enough to feel “the full weight of it,” knowing he was witnessing what would likely happen to him someday.
“Obviously your grandmother dies, you get depressed, but I wasn’t just sad about my grandmother dying. I also started feeling really unmotivated about my future,” he said. “I thought why should I try in school or think about what I want to be when I grow up when it could all just get pulled out from under me at any moment.”
When Should You Get Tested for Li-Fraumeni Syndrome?
Li-Fraumeni syndrome is one of at least 100 cancer predisposition syndromes caused by genetic mutations passed down from parent to child. After learning about these syndromes at a conference, Chenia’s mother, Denese Gascho, decided to have both her children tested due to the family history of cancer on their father’s side, which in addition to Chenia’s grandmother and aunt included his great uncle who died from cancer when he was in his 20s.
More typically, a doctor may recommend an individual or family members get tested for Li-Fraumeni syndrome after a cancer diagnosis, should they meet what is called the “Chompret criteria.” These criteria consider if an individual:
- was diagnosed with a Li-Fraumeni syndrome-associated cancer before the age of 46 and has a first- or second-degree relative who was diagnosed with a Li-Fraumeni syndrome-associated tumor, except breast cancer, before the age of 56 or had multiple tumors;
- had multiple tumors with at least two being Li-Fraumeni syndrome-associated tumors, except if the two tumors are breast cancer, and the first diagnosis occurred before 46;
- was diagnosed with adrenocortical carcinoma, choroid plexus carcinoma, or embryonal anaplastic subtype rhabdomyosarcoma, independent of family history; or
- was diagnosed with breast cancer before the age of 31.
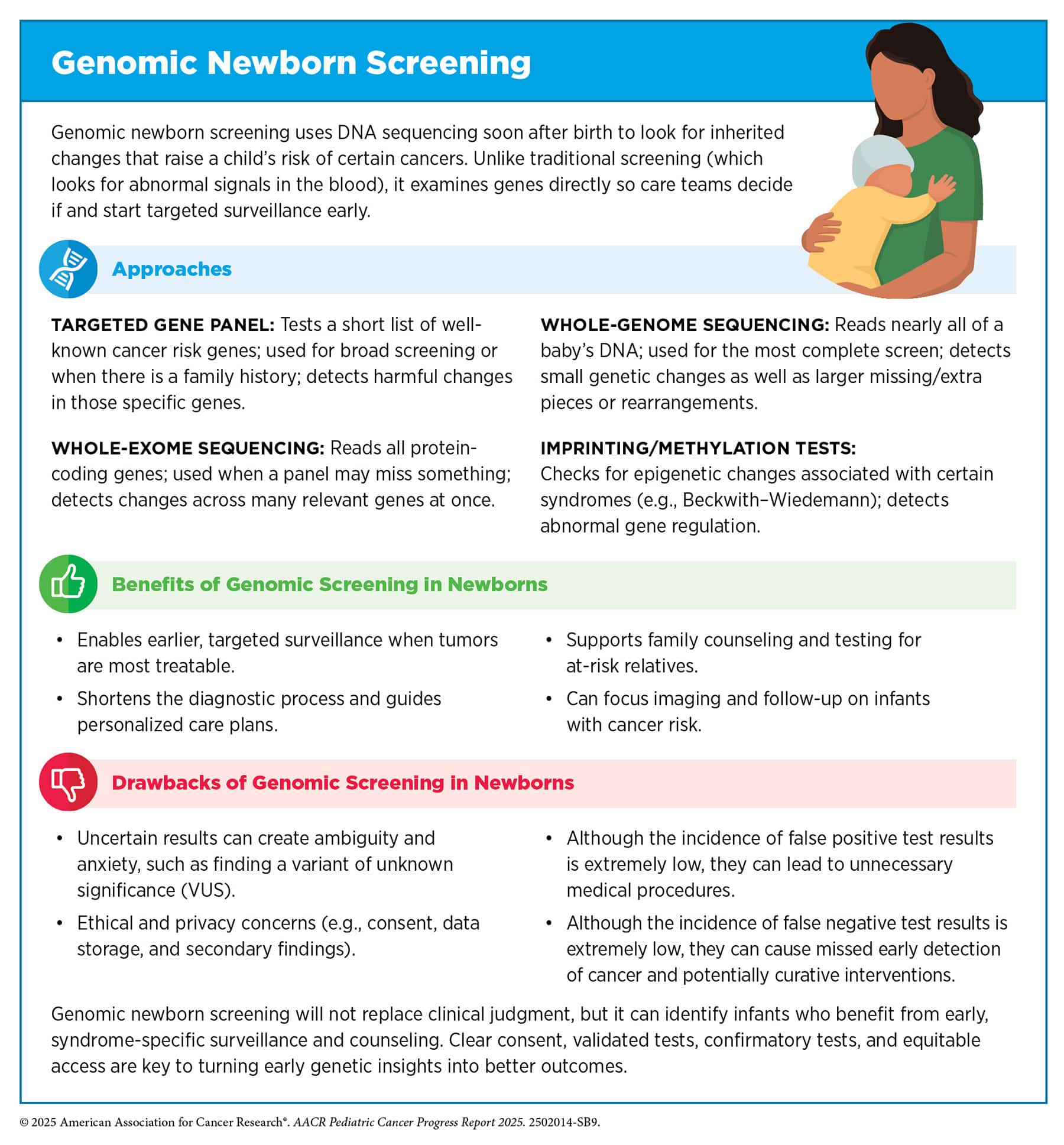
The potential of screening newborns for cancer predisposition syndromes has also been gaining attention, which Sharon E. Plon, MD, PhD, of Baylor College of Medicine, discussed during the Presidential Select Symposium on “Targeting Stage 0: Precision-Based Prevention” at the AACR Annual Meeting 2026. Plon highlighted how every baby is already getting a quality heel stick within 48 hours of birth to test for about 50 to 60 conditions—but not cancer. She pointed to a simulation model that found if newborns were screened for cancer predisposition syndromes, it could decrease deaths from cancer overall by 54% and decrease cancer death before the age of 20 by 8%.
Plon and colleagues will further evaluate the cost, feasibility at scale, and acceptability among parents in implementing newborn genomic screening for cancer predisposition syndromes through studies including the N-CARE randomized clinical trial and Building Evidence and Collaboration for GenOmics in Nationwide Newborn Screening (BEACONS).
“This provides exciting new opportunities for cancer prevention research in children,” Plon said.
The AACR Pediatric Cancer Progress Report 2025 outlines some of the benefits and drawbacks of genomic screening for newborns as well as the role of genetic counseling to help guide families in making the right decision for them. Genetic counseling includes experts in clinical genetics, cancer care, and psychosocial care who help parents understand the options for genetic testing, a child’s risk of cancer if they are diagnosed with a cancer predisposition syndrome, and the recommended protocols to help catch cancers in these children early.
What Are the Cancer Screening Guidelines for Li-Fraumeni Syndrome?
In 2016, the AACR Pediatric Cancer Working Group (PCWG) convened a Childhood Cancer Predisposition Workshop to recommend consistent surveillance protocols to monitor for cancer in children with these syndromes. The group reconvened in 2023 to evaluate how these protocols were working and if they could be improved. The resulting recommendations were published as a series of articles in the AACR journal Clinical Cancer Research.
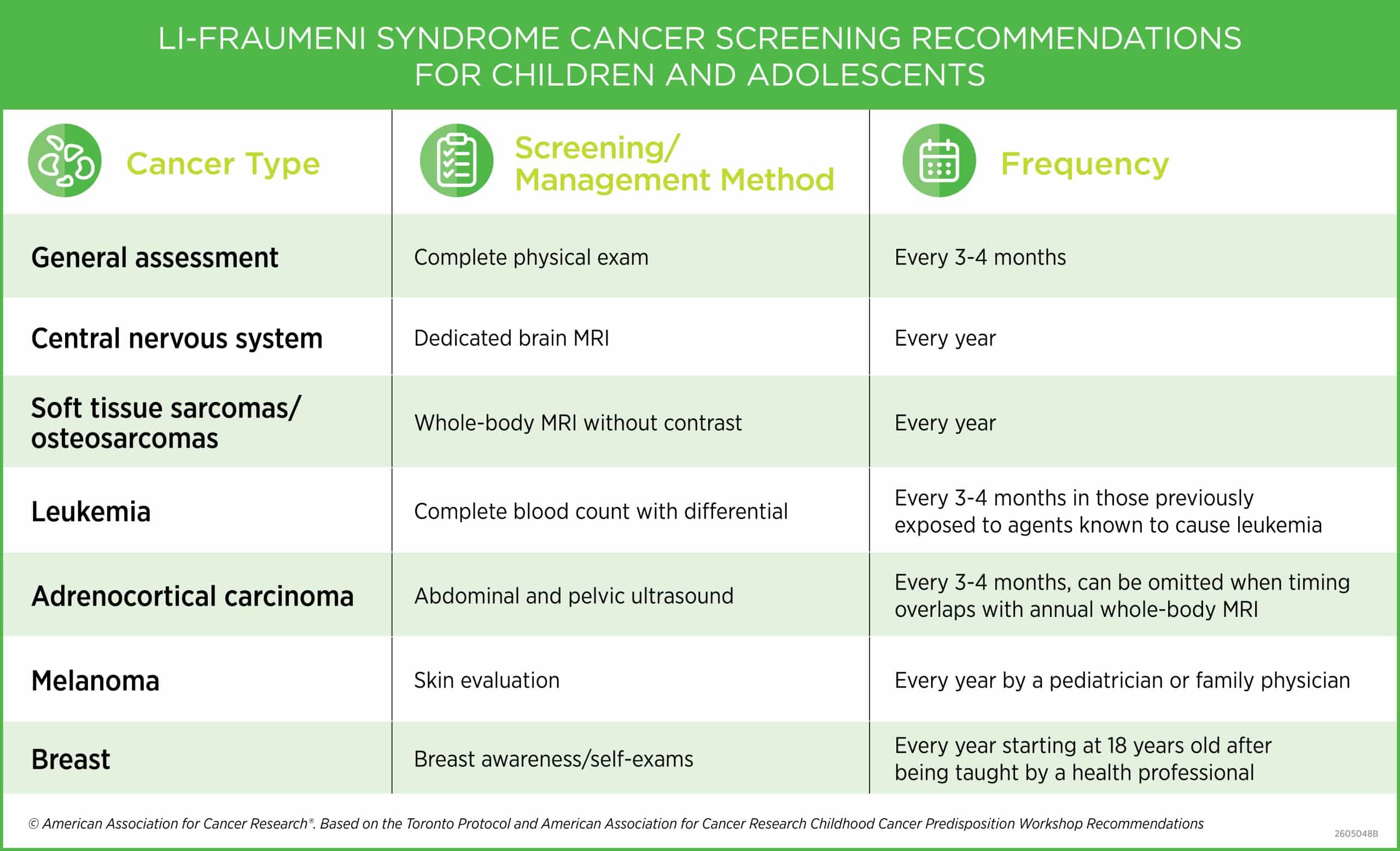
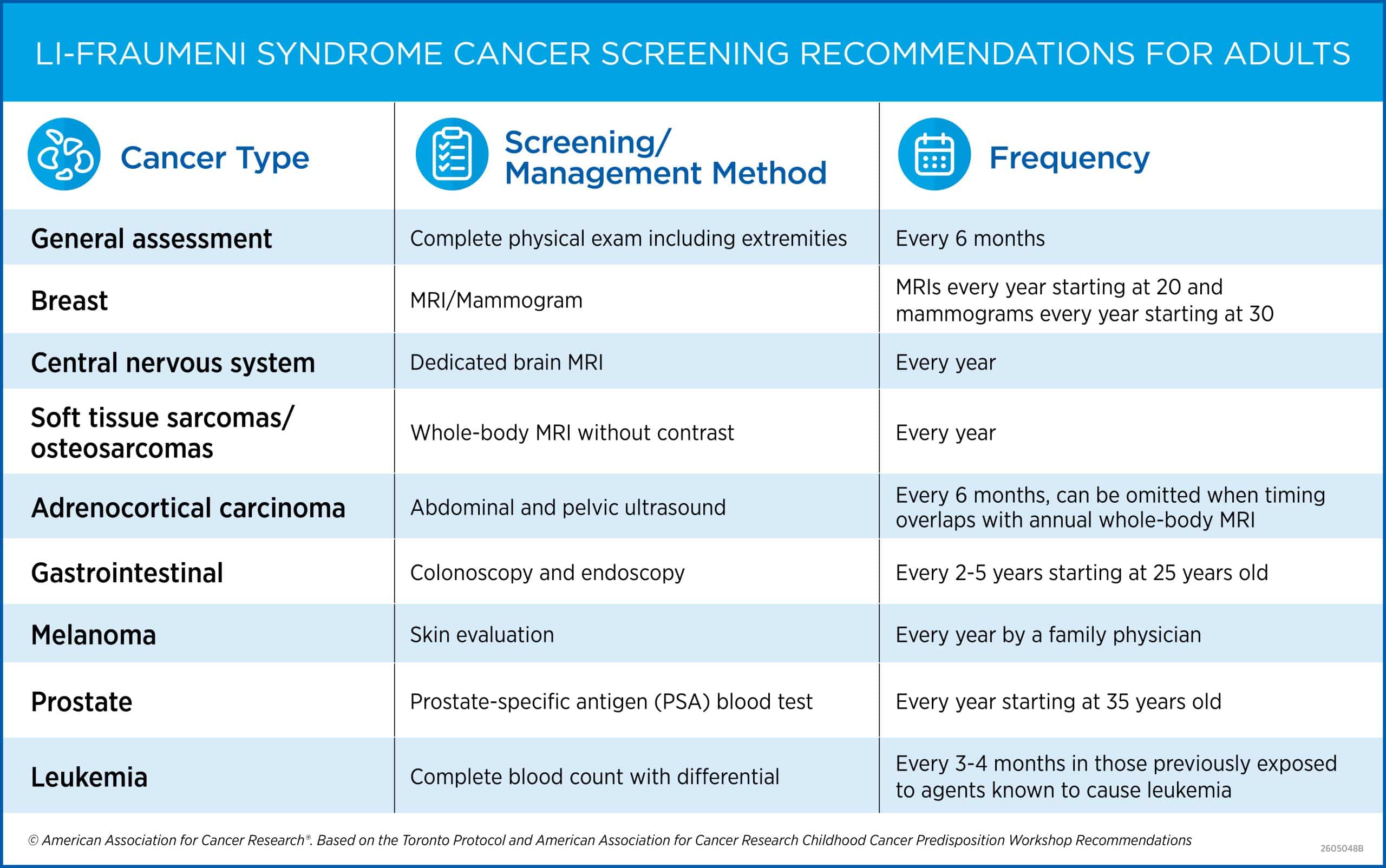
For Li-Fraumeni syndrome, the PCWG recommended following the “Toronto Protocol,” which was established by Malkin and his colleagues at Toronto’s Sick Kids Hospital in 2011, along with a few slight modifications. The guidelines are broken down between screening for children and adolescents (18 and under) and adults (older than 18).
For children and adolescents, screening includes a general assessment from a primary care physician every three to four months with special attention paid to clinical features that are common for Li-Fraumeni syndrome-associated cancers, such as palpable masses, a limp or abnormal gait, persistent pain, frequent headaches, a significant increase in height, unintentional weight loss, etc. Other tests can include dedicated brain MRIs, whole-body MRIs, pelvic ultrasounds, complete blood counts (CBCs) with a differential, skin exams, and self-exams for breasts (starting at 18).
Adults are advised to continue to undergo those same tests with a few additions, including starting breast MRIs and mammograms, colonoscopies and endoscopies, and prostate-specific antigen (PSA) tests at younger ages than recommended for the general population. For adults or children in resource-constrained settings without access to whole-body MRIs, the PCWG recommends any nonradiation-based imaging test that can be cost-efficiently performed as a potential alternative. As for individuals with mosaic Li-Fraumeni syndrome, the PCWG does not recommend modifying guidelines until potential changes have been validated in large studies.
“How I feel about the screenings kind of depends on the day,” Chenia explained, adding that the trips to the hospital can wear him out, which makes them particularly burdensome on days he is busy with school, work, or just life. Plus, there is the anxiety they cause.
“Sometimes I am just freaking out,” he said. “I’m going crazy with what could be happening. And then I go in and I have an MRI and they’re like, ‘Everything’s normal.’ And I just feel so much better.”
That wasn’t the case in late 2021 when his brain MRI found a lesion. A biopsy would confirm that it was a grade 2 astrocytoma, a type of slow-growing glioma, with an IDH mutation. “When my mom called and told me that they had found some sort of mutation, at first, I didn’t process it,” said Chenia, who was 14 at the time. “Days later, I realized—this means I have cancer.”
How Beneficial Is Cancer Surveillance?
The AACR Pediatric Cancer Progress Report 2025 cited several studies that underscore the value of structured cancer surveillance. In one long-term study, 84% of individuals with Li-Fraumeni syndrome who underwent the recommended cancer screening methods and developed cancer were alive at four-year follow-up compared with 49% who were not under surveillance.
In another study, 92% of children who underwent surveillance with an MRI were diagnosed with low-grade brain tumors prior to any symptoms, while 85% of children not under surveillance who were diagnosed after symptoms appeared had high-grade brain tumors. Further, all the children with low-grade tumors who went on to have them surgically removed were alive at 30 months compared with only half of those who were diagnosed with high-grade tumors.
Because Chenia’s tumor was slow growing and caught early through cancer surveillance, his doctors recommended laser ablation. This procedure, which uses focused heat to destroy tumor tissue, took a toll on Chenia.
“I couldn’t tell where my hands or feet were in space,” Chenia said. “I kept bumping into walls. It was funny for like an hour, then it wasn’t.”
The recovery process also drained him of his energy, causing him to fall into what he described as a depressive cycle of going home after school and passing out on his bed. While he had friends to support him, he was too afraid to explain how he was feeling and would often ignore their calls or texts.
“I thought, ‘I’m the worst friend ever,’ but I was going through a rough time,” Chenia explained.
The procedure was successful, but it did not destroy all the cancer. Fortunately, on Chenia’s 17th birthday, his doctor informed him he qualified for an emerging targeted therapy called vorasidenib, an IDH inhibitor that would go on to be approved by the U.S. Food and Drug Administration under the brand name Voranigo in August 2024. The drug was designed to slow tumor growth and has kept Chenia’s tumor stable.
“This treatment gave me my child back,” Denese said. “It means Chenia can go to school, see friends, live life—and not face another surgery.”
How Important Is Mental Health for Individuals With Li-Fraumeni Syndrome?
Chenia’s perspective on life is so much brighter and more hopeful now, thanks in part to vorasidenib, but also the mental health support he received following his cancer diagnosis.
“I believe mental health should be standard for anyone with Li-Fraumeni syndrome,” Chenia said. “It just weighs on you so much.”
Mental health support also helped when yet another member of his family died from cancer—his father. Christopher Paul Gascho passed away from grade 4 glioblastoma in April 2026 after undergoing treatment for almost exactly a year.
“It really shook me because he had been doing everything right,” Chenia said. “He did all the recommended monitoring; he actually had an MRI a few weeks prior to getting diagnosed so it really had grown incredibly quickly.”
Chenia said while his grandmother was in hospice for several months before passing away, everything with his father progressed much faster. And Christopher started to get worse just as Chenia was dealing with final exams at the end of his first year at the University of Toronto, which made it difficult to put his life on hold.
“I regret not seeing him more. I thought I had more time,” Chenia said. “Mental health support has been indispensable through this time. Even aside from the support I’ve received directly after my dad’s passing, the ongoing therapy I’ve been getting for the past several years has given me skills to help me process my feelings in a much healthier way.”
Now, even when he is exhausted by his treatment or trips to the hospital, he is open and honest about it with his friends. He is focused on eating healthy and exercising to not only help him feel better in the present but to have a good quality of life as long as possible. He is dedicated to making sure he spends time with his family.
And he is thinking about his future.
He is studying civil engineering to fulfill his goal to one day design cities and improve public transportation systems.
“I’m now able to live with cancer,” Chenia said. “It doesn’t feel like a thing that happens to you right before you die. It’s a difficult piece of my life, but it is a part of my life and not just the thing that kills me.”


