Stopping Cancer Before It Starts in Lynch Syndrome
Most cancers are driven by sporadic mutations that are acquired at a certain point in a person’s life. These mutations, known as somatic mutations, occur in nonreproductive cells of the body and are not passed down through generations. However, a small proportion (up to 10%) of cancer cases are hereditary, being caused by genetic alterations that are present in every cell of the body, including germ cells, and can be transmitted from parent to child.
These mutations confer predisposition to certain cancer types, which tend to run in families of carriers with higher frequency than in the general population, and to occur early in life.

One of the most common hereditary cancer syndromes is Lynch syndrome. People with this condition are more likely to develop colorectal, endometrial, ovarian, and other cancers. For these individuals, risk reduction is key. The U.S. Centers for Disease Control and Prevention recommend frequent cancer screening to find cancer early when it is more treatable.
Research into the mechanisms and effects of the genetic mutations associated with Lynch syndrome has enabled scientists to devise prevention and interception strategies to thwart cancer development in its earliest stages in people who carry the mutations. Some of these approaches are currently in clinical development and were highlighted at the AACR Annual Meeting 2026, held April 17-22.
Framing the Mutations That Cause Lynch Syndrome
Lynch syndrome is caused by mutations in one of a group of five genes that encode for DNA mismatch repair (MMR) proteins, whose job is to find and repair errors that spontaneously occur during DNA replication. Just like words are composed of letters of the alphabet, genes are made up of a sequence of basic building blocks called nucleotides, which are organized as base pairs in the DNA double helix. The MMR system serves as a “spell-checking” mechanism ensuring that the sequence of base pairs is correctly preserved to maintain accuracy of the information. In cells that don’t have a functioning MMR system, “typos” introduced during DNA replication are not corrected, and errors accumulate, generating mutations. If these mutations occur in critical cancer-associated genes, they can lead to unchecked cell proliferation and malignancy.
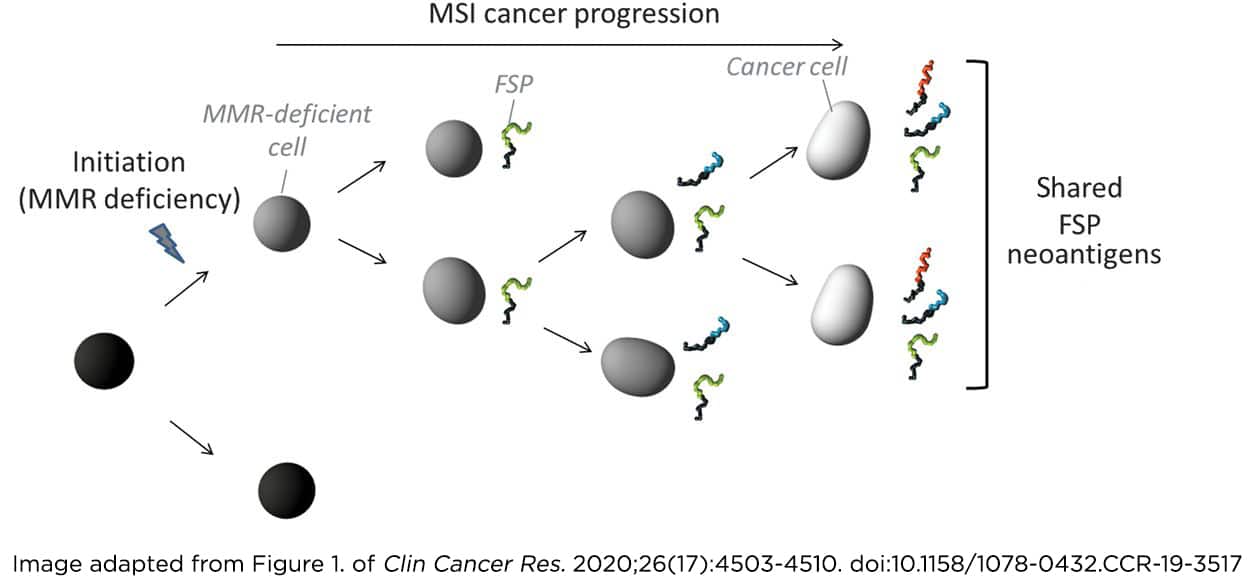
Replication errors in MMR-deficient cells occur more frequently at repetitive genomic sites, such as microsatellites. These are stretches of DNA where a short sequence of base pairs is repeated multiple times, making them particularly tricky to replicate accurately. For this reason, they can become hotspots for frameshift mutations, which disrupt the “frame” through which the coding sequence of a gene is read to make the corresponding protein.
In fact, genes provide a blueprint for the cell to manufacture proteins by assembling building blocks called amino acids in the appropriate sequence. Frameshift peptides (FSPs) are short chains of amino acids produced when the genetic message is decoded incorrectly due to frameshift mutations.
Because frameshift peptides (FSPs) are specific to the tumor cells and are not known to the immune system, researchers reasoned that they could take a similar approach to commonly used vaccines, where a component from an infectious agent is introduced in the body to trigger an immune response against the pathogen. Similarly, FSPs can be leveraged as antigens to train the immune system to recognize and attack precancerous lesions before they develop into cancer. In addition, the mutation hotspots are predictable and shared across different individuals with Lynch syndrome mutations, leading to the idea of an “off-the-shelf” vaccination strategy that could be used to immunize carriers and intercept tumor development.
This approach was discussed during the Presidential Select Symposium on “Targeting Stage 0: Precision-Based Prevention” at the AACR Annual Meeting 2026 as an ingenious example of preventative cancer vaccination. “How would you develop a prophylactic vaccine where you didn’t have the tumor, and you couldn’t pick the antigens from the tumor?” asked presenter Mary (Nora) L. Disis, MD, a professor at the University of Washington. One way, she pointed out, is to find and leverage commonalities across the tumors that may develop in individuals who are genetically at high risk. “One of the commonalities in this group of tumors when they arise is that they develop frameshift mutations,” said Disis.
A Vaccine to Prevent Hereditary Colorectal Cancer
Researchers demonstrated that frameshift mutations translate into immunogenic neoantigens and that an FSP-based vaccine was safe and effective at inducing immune responses in patients with advanced MMR-deficient colorectal cancer. Shifting this approach toward cancer prevention, a study conducted in a preclinical model of Lynch syndrome, which was presented at the AACR Annual Meeting 2019, showed that a preventive vaccine encoding four FSP neoantigens led to reduced intestinal tumor burden and prolonged survival in mice, providing proof of concept for further development of FSP vaccination efforts for cancer prevention in people with Lynch syndrome.
In the new study highlighted by Disis at the Annual Meeting this year, the authors ran a phase Ib/II clinical trial to evaluate Nous-209, a vaccine encoding 209 FSP neoantigens that are common in MMR-deficient tumors. The vaccine was delivered using viral vectors to stimulate strong CD4+ and CD8+ T cell responses against the neoantigens. By including a high number of neoantigens, the researchers hoped to maximize the likelihood of inducing a broad T-cell response against shared mutations across a wide patient population.
When given to individuals with Lynch syndrome with no signs of cancer for at least six months before vaccination, Nous-209 was well tolerated and elicited strong and long-lasting T-cell responses against the FSP neoantigens. Furthermore, at the time of analysis (13 to 17 months after the first vaccination shot), 21 out of 43 evaluable participants had not developed any colorectal adenomas, and no cases of advanced adenoma were found, suggesting early evidence of tumor interception. A commentary published in Cancer Discovery, a journal of AACR, provides a more extensive discussion of the Nous-209 vaccine and the next steps in the path toward a preventive cancer vaccine for people with Lynch syndrome.
Fine-tuning Aspirin Dosage for Cancer Prevention
The National Comprehensive Cancer Network recommends considering daily aspirin intake for prevention of colorectal cancer in individuals born with Lynch syndrome, based on the results of the large randomized CAPP2 clinical trial. After a 10-year follow-up period, this study demonstrated that a daily dose of 600 mg of aspirin resulted in a 35% lower risk of developing colorectal cancer, with the protective effect emerging after five years of treatment and persisting for up to 20 years. However, despite the clinical guidelines, aspirin use for cancer prevention in this population is not very common, due to concerns about potentially serious side effects such as bleeding. The researchers conducted another trial, CaPP3, to investigate whether lower doses of aspirin had the same cancer prevention effect.

During the Presidential Select Symposium, John Burn, MD, a professor at Newcastle University in the United Kindgom, discussed the results of the CaPP3 study. A dose of 100 mg of aspirin, which is comparable to that prescribed for individuals with cardiovascular risk, was as effective as 600 mg in reducing colorectal cancer incidence in people with Lynch syndrome with no serious adverse events, Burn reported.
The mechanism through which aspirin prevents colorectal cancer has not been entirely elucidated and is thought to be related to inhibition of inflammation. However, Burn explained that a low dose of 100 mg is not enough to inhibit the COX-2 enzyme. Further research is focusing on the role of the mTOR cell signaling pathway and on the ability of aspirin to promote apoptosis. According to Burn, the most exciting results concern the antiplatelet effect of aspirin through inhibition of the COX-1 enzyme, which blunts the production of an immune suppressive molecule and results in enhanced antitumor T-cell responses.
Based on the findings from CaPP3, Burns opined that low-dose aspirin can be recommended to all individuals with Lynch syndrome starting five years before colonoscopy and stopping at 70 years old, at which age the side effects become higher and the protective effect potentially lower.
AACR Annual Meeting sessions are available for virtual viewing for all registered attendees through October 2026.