The Long Road to Receiving Care—Examining Cancer Disparities in Rural Areas
After turning 55, Dennis Gruenhagen retired to a remote spot in rural Wyoming where his closest neighbors were 2 miles away. He built a home from the ground up, and cared for cattle, horses, and goats. But when he was diagnosed with amyloid light-chain amyloidosis in his late 70s, his local providers—who were 60 miles away—were limited in the care they could offer. They referred him to the Mayo Clinic in Rochester, Minnesota, where he was enrolled in a clinical trial. This meant he had to travel 680 miles every two weeks to receive treatment.
“No doubt the easiest thing would have been for me to move real close to Rochester, but I loved it out in Wyoming too much,” Gruenhagen shared in the AACR Cancer Disparities Progress Report 2026. “I would have been without my animals and things like that, and I couldn’t part with that.”
Gruenhagen’s story is just one example from the AACR Cancer Disparities Progress Report 2026 that highlights the impact geography can have on cancer care. Released every two years, this report features the latest statistics on both the progress being made against cancer disparities and the continued disproportionate toll that cancer exacts on medically underserved populations, including racial and ethnic minority groups, sexual and gender minorities, and residents of rural areas like Gruenhagen.
Based on one 30-year analysis, the report details how U.S. patients in rural areas traveled an average 2.5 times farther than patients in urban areas to access a clinical trial. This situation is only getting worse as 193 rural hospitals have closed in the past two decades due to financial pressures. As of 2022, more than 70% of U.S. counties had no active cancer clinical trials, with 86% of nonmetropolitan counties lacking a trial compared with 44% of metropolitan counties. Additionally, as of 2024, only 7% of U.S. oncologists worked in rural areas where nearly 16 million adults 55 or older reside.
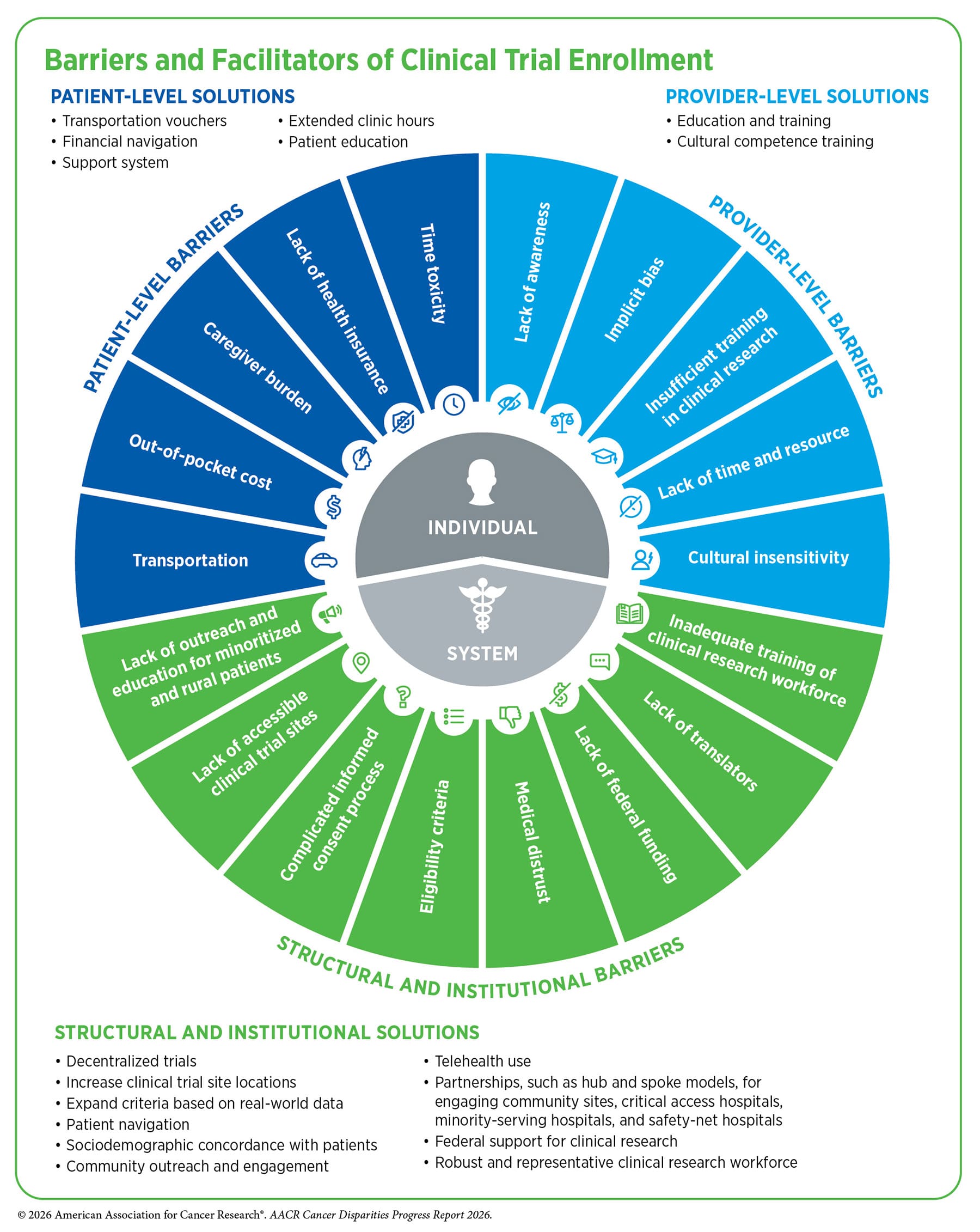
The report notes that researchers and lawmakers are working to address these disparities through several strategies, including decentralized clinical trials where rural hospitals partner with major health networks or academic cancer centers, greater utilization of telehealth, and offering financial and travel support. For example, the Mayo Clinic provided Gruenhagen with transportation assistance, so he would only need to drive halfway to Chamberlain, South Dakota, to meet a ride that would take him the rest of the way.
“I couldn’t have done it without it,” Gruenhagen said. “It was just too much.” He explained how grueling it was to even drive 300 miles each way, especially when he had to deal with harsh weather or change a flat tire on the interstate, but he persisted. After about three years, his treatment proved effective and his doctors declared a complete hematologic response.
Age and other health issues, including heart complications and kidney problems, eventually forced Gruenhagen to relocate to Iowa to be closer to medical care, but he was grateful for the 26 years he got to spend in Wyoming.
“Best years of my life,” he said.
The Growing Gap in Cancer Care Between Rural and Urban Areas
Another issue detailed in the AACR Cancer Disparities Progress Report 2026 is the increasing disparities in cancer mortality rates. In the 1990s and 2000s, the highest cancer mortality rates shifted from large metropolitan areas in the United States to nonmetropolitan areas, likely due to a geographic redistribution of social determinants of health, including exposure to certain cancer risk factors and access to high-quality cancer screening and treatment.
The report also explains how the rural-urban gap in cancer incidence and mortality is exacerbated for certain types of cancer. For example, between 2019 and 2023, incidence rates were higher in rural areas compared with urban areas for lung (37%), cervical (26%), and colorectal (17%) cancers. Residents in rural areas were also more likely to die from these cancers with death rates 27% higher for colorectal cancer, 32% higher for cervical cancer, and 36% higher for lung cancer. Similar issues have also been found with cancer screenings. For instance, in 2022, women in rural areas were 14% less likely to be up to date on breast cancer screenings compared with those in urban areas.
“A common thread across all cancer disparities is access. When access improves, survival improves,” AACR Cancer Disparities Progress Report 2026 Steering Committee Chair Mariana C. Stern, PhD, said during a congressional briefing where the report was released. Stern, who is a professor and the Ira Goodman Chair in Cancer Research at the Keck School of Medicine of the University of Southern California and associate director of population science at the USC Norris Comprehensive Cancer Center, added how strategies must be implemented to lower barriers to care. For example, the report highlighted the benefits seen from the use of patient navigators within the community, with one such program increasing five-year survival rates for breast cancer by 70%.
Another example of a community outreach program mentioned in the report is the Chickahominy TRUTH (Trust, Research, Understand, Tell, Heal) Project. For this initiative, the VCU Massey Comprehensive Cancer Center partnered with the Chickahominy Tribe to address tribal leaders’ concerns over the growing number of cancer cases among members of their community in the rural area of Charles City, Virginia. While the goal of the project was to help better understand the possible environmental factors that could be contributing to this rising incidence, it also established trust between the tribe and the cancer center.
So, when Melanie R. Stewart, a citizen of the Chickahominy Tribe, was diagnosed with breast cancer on two separate occasions, her daughter, Lindsey Johnson, reached out to Robert A. Winn, MD, FAACR, who was the director and Lipman Chair in Oncology of the VCU Massey Comprehensive Cancer Center at the time. Winn helped Stewart access the care she needed, including nurse navigation that supported her through every step of the process.
“Having Dr. Winn and the entire Massey team genuinely care about our community made an incredibly difficult experience feel more hopeful,” Johnson said.
But Stewart knows that not everyone in her community may have the same opportunities as her. For one, while her daughter was able to help her make the 40-mile trip to the cancer center, there are citizens of the tribe who live farther away and don’t have access to transportation. In other instances, tribal elders may be reluctant to seek care due to mistrust of the medical system. So, to help ensure more individuals have access to care, the Chickahominy Tribe has expanded health-related services, such as in-home nurse visits, transportation assistance, and community health fairs promoting awareness and prevention.
“Everyone deserves health care,” Stewart said.
Seeking Answers Across the Country
Living in a rural area is not the only geographical barrier patients may face. When Michael Casaus and Naomi Natale from Albuquerque, New Mexico, learned their then 2-year-old son Sebastián—affectionately called Sebas—had an ultra-rare cancer, myoepithelial carcinoma (MEC), they were desperate for answers. But their local care team had never treated a patient with this disease. Even consulting with specialists virtually was difficult because they lived in a state that is not part of an interstate medical licensure agreement. So, they drove four hours to El Paso, Texas, three different times just to sit in a parking lot to consult with a specialist over Zoom.
“It’s a very lonely feeling to know that your son was diagnosed not only with cancer, but also with an ultra-rare cancer that nobody knows anything about,” Casaus said. “We really felt like we were stepping into darkness.”
There were no standard protocols and very little research to guide care decisions. While doctors recommended chemotherapy based on a small study involving seven patients, the ultimate decisions on how to treat Sebas were left up to Casaus and Natale.
“When there’s such limited information, it felt like throwing a dart at a dart board and just seeing what may land,” Casaus said.
Eventually, they decided to relocate their family to California so Sebas could be treated at Lucile Packard Children’s Hospital Stanford by doctors who had previously encountered MEC. But this move required Casaus to take a leave of absence from his nonprofit work, for Natale to quit her teaching position, and for Sebas’ brother, Santiago, to be pulled from preschool.
“Our lives were upended through and through,” Casaus said.
Sebas underwent an intensive treatment course that included multiple rounds of chemotherapy. Although the treatment did not eliminate the cancer, his disease has remained stable and he continues to be monitored with scans every three months, now at the Children’s Hospital of Philadelphia. However, the chemotherapy caused Sebas, now 7, to develop osteoporosis and left him with what Casaus described as “the bones of a 70-year-old.” In 2025, he suffered five fractures just from playing as any child would.
“We can’t shield our son from playing and being a kid, but it scares us every day,” Casaus said.
To help advocate for research funding to find treatments for MEC and to ensure patients and families have access to information about this ultra-rare cancer, Casaus and Natale founded the nonprofit organization cureMEC: The Myoepithelial Carcinoma Project in 2022.
“We learned quickly that families like ours are left to figure it out on their own,” Casaus said. “For kids around the country who are facing this devasting diagnosis, they deserve more.”
The AACR Cancer Disparities Progress Report 2026 concludes with a call to action for policymakers and other stakeholders to sustain and strengthen federal investments in cancer disparities research; ensure equitable cancer prevention, screening, genetic testing, and follow-up care; and implement policies to ensure equitable patient access to lifesaving therapies, among other actions.
“Too many individuals still face barriers to cancer prevention and screening. Too many communities lack access to timely follow-up after an abnormal screening result. Too many patients are never offered the opportunity to participate in a clinical trial. Too many patients live very far from high-quality cancer care. And far too many patients face financial, logistical, cultural, and other structural barriers that continue to shape their chances for survival,” Margaret Foti, PhD, MD (hc), chief executive officer of AACR, said during the report’s congressional briefing. “Addressing cancer disparities requires a national commitment to ensuring that a person’s socioeconomic, geographic, or other factors do not determine whether they will survive a diagnosis of cancer.”
Read the full AACR Cancer Disparities Progress Report 2026 for more information about the disparate burden of cancer across population groups in the United States.
AACR will also hold the 19th AACR Conference on The Science of Cancer Health Disparities from October 18 to 21 in Atlanta, Georgia, which will include a special session about the report. The abstract submission deadline is July 23, and the advance registration deadline is September 8.