
FDA Approvals in Oncology: April-June 2026
During the second quarter of 2026, oncology approvals issued by the U.S. Food and Drug Administration expanded the treatment options available for patients with breast cancer, urinary cancers, prostate cancer, rare cancers, and hematologic malignancies.
Keep reading to learn about these approved therapeutics and how each fits into the treatment landscape of its respective cancer type.
Breast Cancer: First PROTAC, New ADC Indications, and More
Almost 322,000 women are expected to be diagnosed with breast cancer this year, but thanks to advances in treatment and early detection, the relative five-year survival in recent years has been over 90%.
Five approvals issued this quarter exemplify the progress that continues to be made against multiple subtypes of this disease, including a new treatment modality and the expanded use of antibody-drug conjugates (ADCs).
HR-positive, HER2-negative Breast Cancer
About 70% of breast cancers are hormone receptor (HR)-positive and human epidermal growth factor 2 (HER2)-negative. Patients with these cancers are typically treated with endocrine therapy to block estrogen’s cancer-promoting activity in various ways, such as by disrupting estrogen production, blocking estrogen from binding to the estrogen receptor (ER), or destabilizing the ER so that it is ultimately degraded. The latter class of endocrine therapy comprises the selective estrogen receptor degraders (SERDs) fulvestrant (Faslodex), imlunestrant (Inluriyo), and elacestrant (Orserdu).
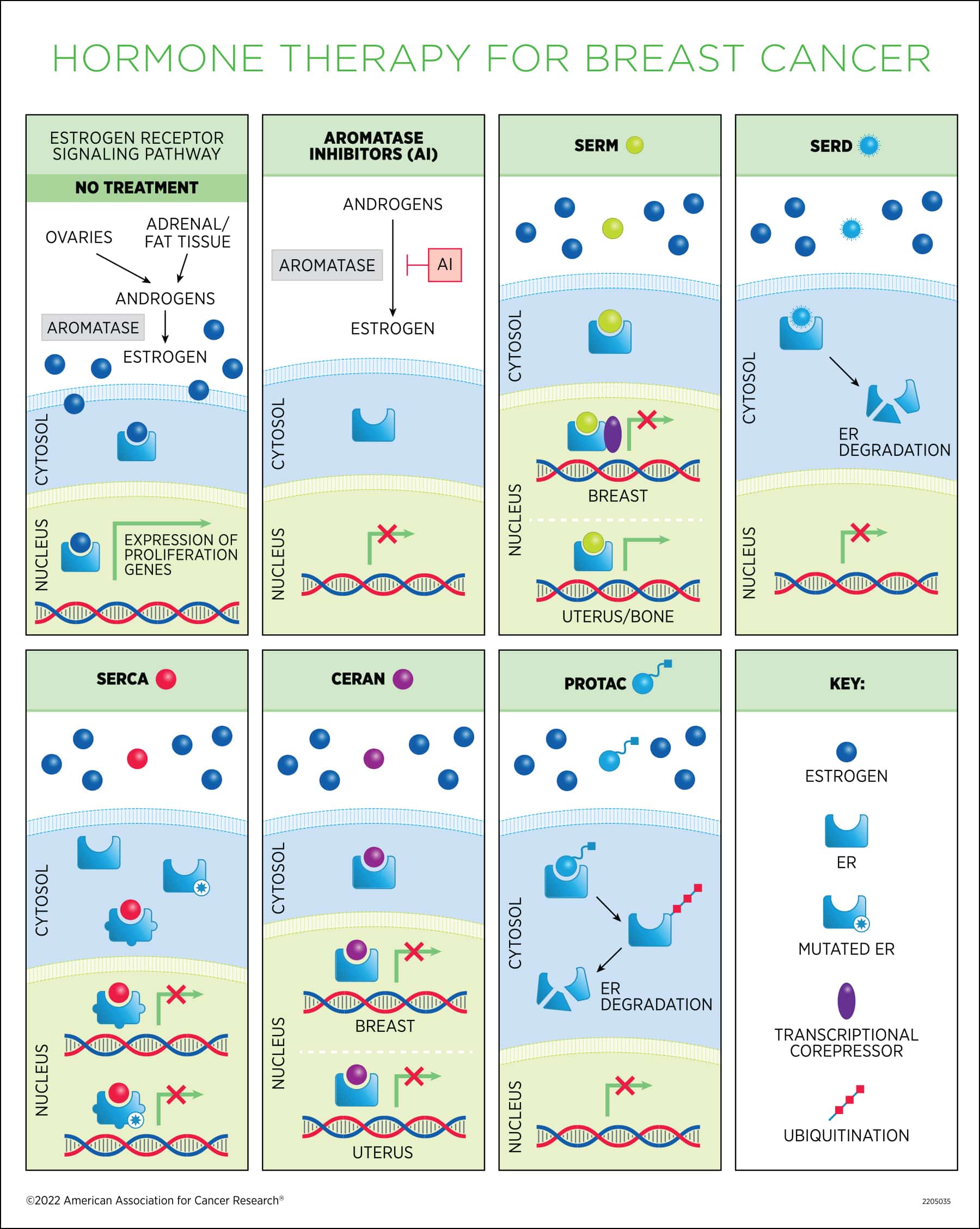
This quarter, the FDA approved a first-in-class therapeutic that degrades the ER through a different mechanism than SERDs.
- Vepdegestrant (Veppanu) was approved to treat ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer that has progressed after at least one prior line of endocrine therapy.
Vepdegestrant is an example of a proteolysis-targeting chimera (PROTAC), a type of small molecule that binds to its target—ER in this case—and brings it to an E3 ubiquitin ligase to actively induce target degradation. Vepdegestrant is the first PROTAC to receive FDA approval for any cancer type.
The approval was based on clinical trial data reported at the San Antonio Breast Cancer Symposium (SABCS) 2025, which is co-organized by the American Association for Cancer Research (AACR). The results showed that among patients whose breast cancers had mutations in the ESR1 gene, which encodes the ER, those treated with vepdegestrant had significantly longer progression-free survival (PFS) than those treated with fulvestrant.
With its approval, vepdegestrant joins imlunestrant and elacestrant as oral ER-degrading therapeutics approved for this patient population.
HR-positive, HER2-positive Breast Cancer
HR-positive breast cancer treated with endocrine therapies frequently become resistant to those treatments, in part due to CDK4/6 activity. Combining endocrine therapy with CDK4/6 inhibition helps overcome resistance, and this combination has been approved for patients with HR-positive, HER2-negative breast cancers.
For patients whose cancers are positive for both HR and HER2, however, no such combination was previously available. This quarter, the FDA approved the first CDK4/6 inhibitor for HER2-positive breast cancers.
- Palbociclib (Ibrance) was approved in combination with the HER2-targeted monoclonal antibody trastuzumab (Herceptin), with or without the HER2-targeted therapy pertuzumab (Perjeta), and endocrine therapy as maintenance therapy for patients with locally advanced or metastatic, HR-positive, HER2-positive breast cancer.
Researchers first reported that adding palbociclib to maintenance therapy improved PFS in this patient population at SABCS 2024. The FDA approval of the regimen was based on updated PFS data from the trial.
HER2-positive Breast cancer
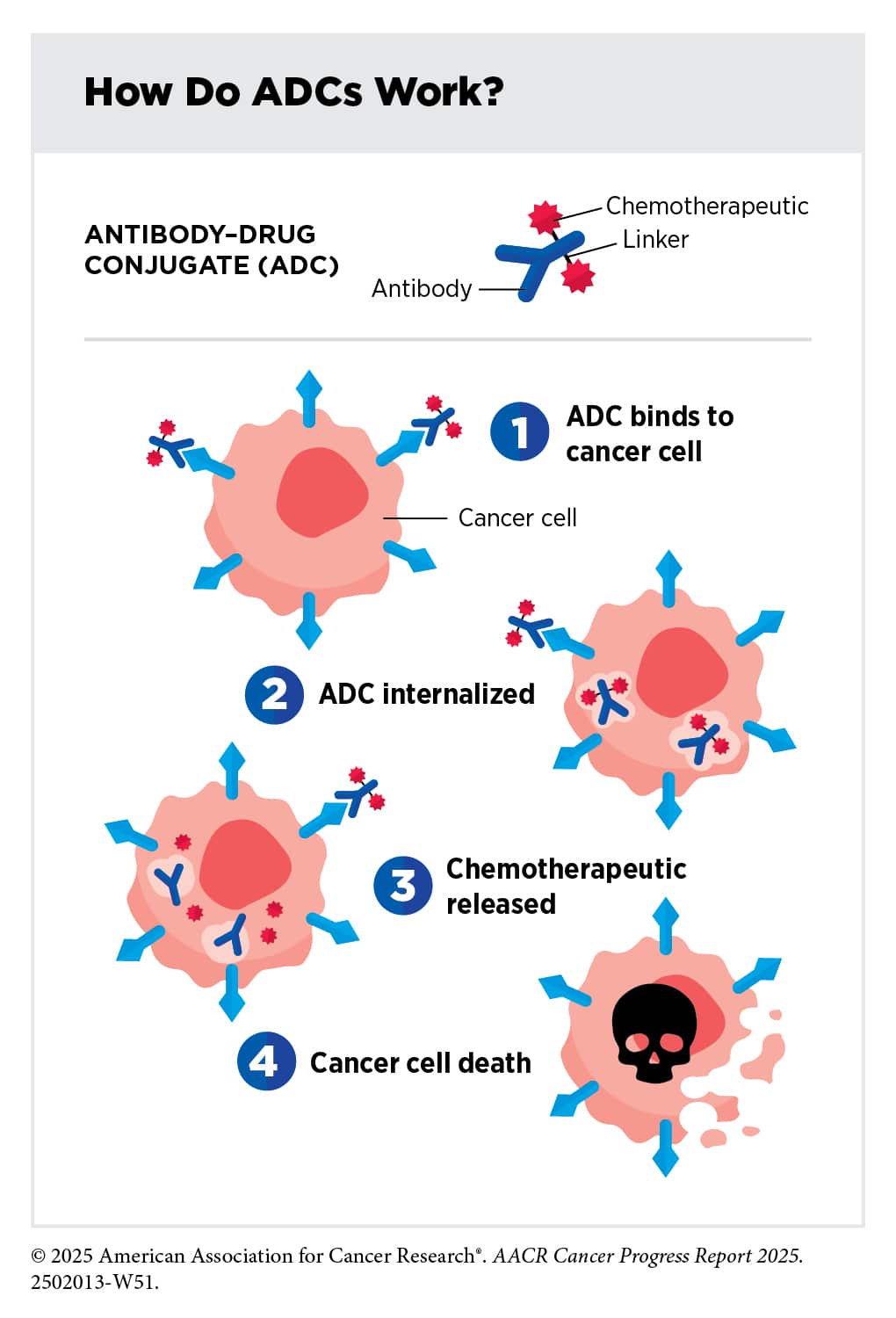
An ADC that delivers a cell-killing drug to HER2-expressing cells, trastuzumab deruxtecan (T-DXd, Enhertu) has been previously approved to treat metastatic, HER2-positive or HER2-low breast cancers. Two new indications approved this quarter mean that T-DXd treatment may now be used for early-stage cancers as well.
- T-DXd was approved for two indications in patients with early-stage, HER2-positive breast cancer:
- as neoadjuvant therapy and followed by neoadjuvant taxane-based chemotherapy, trastuzumab, and pertuzumab for adults with stage 2 or 3 breast cancer; and
- as adjuvant therapy for patients who have residual invasive disease after neoadjuvant treatment with trastuzumab (with or without pertuzumab) and taxane-based therapy.
Triple-negative Breast Cancer
Until recently, the standard first-line treatment available for patients with unresectable or metastatic triple-negative breast cancer (TNBC) was chemotherapy. This is because TNBC does not respond to hormone therapies and HER2-targeted therapies. Although the 2020 approval of the PD-1-targeted immunotherapy pembrolizumab (Keytruda) for metastatic TNBC provided a new first-line option for some patients, most patients with TNBC are ineligible for this therapy due to the lack of PD-L1 expression in their tumors.
This quarter, the FDA approved two alternatives to first-line chemotherapy for patients with metastatic TNBC who are ineligible for PD-1/PD-L1-targeted immune checkpoint inhibitors like pembrolizumab. Both are ADCs targeting the TROP2 protein that is overexpressed by many solid tumors, including TNBC.
- Datopotamab deruxtecan (Dato-DXd, Datroway) was approved for patients with unresectable or metastatic TNBC who are not eligible to receive a PD-1/PD-L1-targeted immune checkpoint inhibitor.
- Sacituzumab govitecan (Trodelvy) was approved for patients with unresectable locally advanced or metastatic TNBC who are not candidates for PD-1/PD-L1-targeted immune checkpoint inhibition. Sacituzumab govitecan was also approved in combination with pembrolizumab for patients with unresectable locally advanced or metastatic TNBC who are eligible for pembrolizumab if their tumors express PD-L1.
Learn more about the emerging role of ADCs as first-line treatment for TNBC in this prior blog post that features perspectives from leading breast cancer experts who discussed TNBC treatment advances at SABCS 2025.
Urinary Cancers: New Systemic Options for Bladder and Kidney Cancers
This past quarter, the FDA greenlit three treatments for cancers arising in the urinary system, a network that produces, stores, and transports urine.
For bladder cancer, two immune checkpoint inhibitors were approved:
- Durvalumab (Imfinzi) was approved in combination with the immune-stimulating Bacillus Calmette-Guérin (BCG) to treat patients with high-risk non-muscle invasive bladder cancer (NMIBC) who have not received prior BCG treatment.
Prior to this approval, patients with NMIBC, an early stage of bladder cancer, were not eligible for immunotherapy unless their tumor did not respond to prior BCG treatment. With durvalumab’s approval, patients can now receive upfront immunotherapy.
- Atezolizumab (Tecentriq or Tecentriq Hybreza) was approved as adjuvant therapy for patients with muscle-invasive bladder cancer (MIBC) who have circulating tumor DNA (ctDNA) after cystectomy, signaling the presence of molecular residual disease (MRD).
Treatment guided by the presence of MRD can help ensure that only patients with residual cancer receive the therapy, thereby sparing ctDNA-negative patients from potential immunotherapy-related toxicity. While MRD has been used to guide therapy for hematologic cancers, this is the first FDA approval for a solid tumor to include a requirement for ctDNA positivity.
The FDA also approved a treatment for certain patients with kidney cancer:
- Belzutifan (Welireg) was approved in combination with pembrolizumab as adjuvant treatment for patients with clear cell renal cell carcinoma that has an intermediate-high or high risk of recurring. The combination was also approved as adjuvant treatment for patients who had surgery to remove metastatic lesions.
Belzutifan inhibits hypoxia-inducible factor-2α, a transcription factor that helps cells adapt to low-oxygen environments, such as those found within tumors. It was previously approved as a monotherapy for von Hippel-Lindau disease with associated clear cell renal cell carcinoma or for advanced clear cell renal cell carcinomas that had progressed after prior treatment with an immune checkpoint inhibitor and antiangiogenesis agent. The latest approval expands belzutifan’s reach to patients with earlier stages of disease who have not received prior immunotherapy or antiangiogenesis therapeutics.
Prostate Cancer: Targeted Therapy for Metastatic Castration-sensitive Disease
In the United States, one out of every eight men will be diagnosed with prostate cancer during their lifetime. Fortunately, most cases are diagnosed at early stages, when the cancer is more easily treated, but nearly 10% of cases are diagnosed after their prostate cancer has already metastasized. For these metastatic cases, hormone therapy has long been the mainstay of treatment. An approval issued this past quarter offers a new, more targeted option.
- Capivasertib (Truqap) was approved in combination with the androgen-targeting drug abiraterone (Zytiga) and the steroid prednisone for patients with PTEN-deficient, metastatic prostate cancer that is either susceptible to androgen pathway modulation or that has not yet been treated with an androgen pathway-modulating therapy. These cancers are known as metastatic androgen pathway modulation-naïve or -sensitive (mAPMN/S) prostate cancer.
Capivasertib is an inhibitor of AKT, a signaling protein that promotes tumor growth. PTEN is an upstream protein that normally keeps AKT activity in check, but in PTEN-deficient cancers, AKT remains active and drives cancer progression.
Rare Cancers: Targeted Treatments Expand Options
Patients with rare cancers often face limited treatment options, but FDA approvals issued this past quarter are expanding options for these patients.
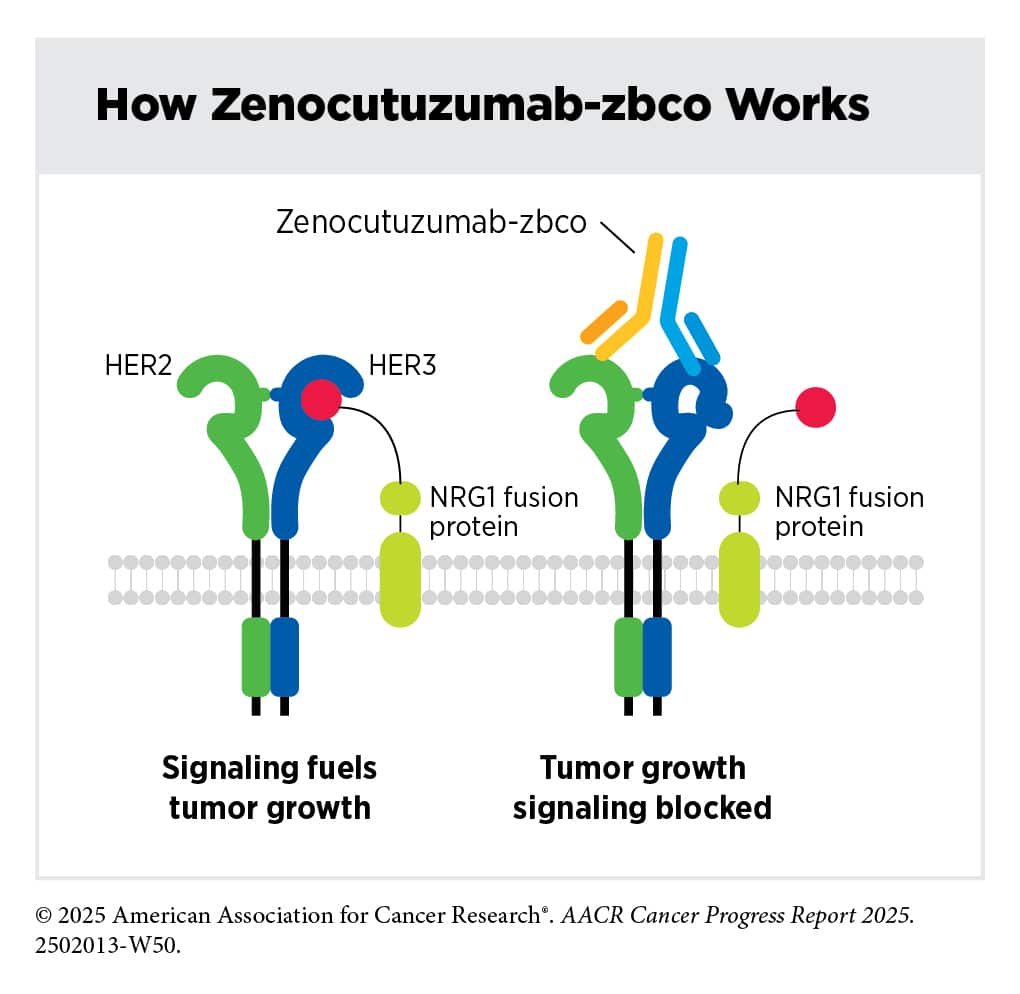
- Zenocutuzumab (Bizengri) was approved for patients with advanced, unresectable or metastatic cholangiocarcinoma harboring a neuregulin 1 (NRG1) gene fusion that has progressed after prior systemic therapy.
NRG1 gene fusions lead to the production of a fusion protein that drives tumor growth by facilitating the formation of the HER2-HER3 complex. Zenocutuzumab is a bispecific antibody that targets both HER2 and HER3, blocking the formation of the HER2-HER3 complex. The clinical trial results that led to the FDA approval were reported at the 2025 AACR-NCI-EORTC International Conference on Molecular Targets.
Cholangiocarcinomas are typically treated with first-line chemotherapy and immunotherapy, but disease progression is common. The approval of zenocutuzumab offers a second-line treatment option for patients with NRG1-fusion-positive cholangiocarcinoma, whose tumors tend to lack other actionable targets.
- This quarter, the FDA converted the 2024 accelerated approval of afamitresgene autoleucel (Tecelra) for certain adults with unresectable or metastatic synovial sarcoma to a traditional approval. The FDA also expanded the indication to include pediatric patients aged 12 and older. For adults and children, the therapeutic is approved for patients who have received prior chemotherapy; test positive for the HLA haplotype A02:01P, A02:02P, A02:03P, or A02:06P; and whose tumor expresses the MAGE-A4 protein.
The FDA’s Accelerated Approval Program allows treatments to receive accelerated approval based on surrogate endpoints that can provide early support for a treatment’s efficacy. When an accelerated approval is converted to a traditional approval, it means that follow-up clinical testing confirmed that the treatment provides clinical benefit.
Afamitresgene autoleucel was the first approved T-cell receptor (TCR) T-cell therapy, a type of cellular immunotherapy in which patients’ T cells are harvested, engineered to better fight their tumor, and infused back into the patient’s body. It was also the first cellular immunotherapy approved for synovial sarcoma.
The therapeutic targets MAGE-A4, which is expressed by many tumors, including synovial sarcomas. Only certain HLA proteins can present MAGE-A4, so afamitresgene autoleucel is approved only for patients who have such an HLA.
- Pivekimab sunirine (Decnupaz) was greenlit to treat patients with blastic plasmacytoid dendritic cell neoplasm (BPDCN), a rare hematologic malignancy.
Patients with BPDCN tend to be older and more susceptible to chemotherapy-related toxicity, limiting their treatment options. Pivekimab sunirine is an ADC that targets CD123, which is universally expressed by BPDCN cells, to deliver a DNA-damaging agent.
Leukemia and Lymphoma: A Second-generation Inhibitor and Oral Chemotherapy
The second quarter of 2026 also brought three more approvals for hematologic malignancies.
- Sonrotoclax (Beqalzi) received accelerated approval to treat mantle cell lymphoma (MCL) that is refractory to or relapsed after two or more prior lines of systemic therapy that included a Bruton’s tyrosine kinase (BTK) inhibitor.
Patients with relapsed/refractory MCL face poor prognoses and have few treatment options. Sonrotoclax is a second-generation inhibitor of the protein BCL-2. This protein is overexpressed in MCL, where it prevents cell death and promotes tumor growth. This is the first FDA approval for sonrotoclax, which is designed to overcome limitations of venetoclax (Venclexta), a first-generation BCL-2 inhibitor.
- Decitabine and cedazuridine tablets (Inqovi) were approved in combination with venetoclax to treat acute myeloid leukemia (AML) in patients who are at least 75 years old, or who are not eligible for intensive induction chemotherapy.
Decitabine and cedazuridine are both chemotherapy agents that kill cancer cells by inducing changes to DNA. The orally administered tablets enable patients to receive the treatment at home, rather than having to travel to receive infusions of previous standard-of-care regimens. - Allogeneic regulatory T-cell-based immunotherapy with hematopoietic stem and progenitor cell (HSPC) and T cells (Tregzi) was approved for patients with hematologic malignancies undergoing hematopoietic stem cell transplantation with a preparative regimen that destroys the cells in their bone marrow.
Unlike traditional hematopoietic stem cell transplants, in which only HSPCs are transferred, this treatment involves infusions of three different cell types: HSPCs, regulatory T cells, and conventional T cells. It is the first approved immunotherapy to use regulatory T cells, a subset of immune cells that help keep the immune system in check. The treatment is intended to help the patient’s cells recover after the pretransplant preparative regimen and to reduce the patient’s risk of developing chronic graft-versus-host disease, which is a complication that can occur after a stem cell transplant.
Check out our FDA approvals page for a comprehensive overview of each oncology approval, including the clinical data that led to each.

