AACR Annual Meeting 2017: Panel Discusses the Affordable Care Act
Chiara D’Agostino had a feeling she would benefit from the Affordable Care Act (ACA). A former Italian teacher, she had given up her full-time job to pursue a graduate degree.
She applied for coverage under the ACA in June 2014, then spent the summer studying in Italy. When she came home, she went for her yearly physical and got a clean bill of health. Because she was in her early 40s, she also went for a mammogram. Another clean bill of health.
In September, she received notice that she’d been approved for coverage under the ACA. And in October, she discovered a lump in her breast. She was soon diagnosed with stage 3 triple-negative breast cancer, an aggressive form of the disease that is notoriously difficult to treat.
Since then, she has had two mastectomies, multiple reconstructive surgeries, biopsies, chemotherapy, and radiation. Her cancer metastasized and is now considered stage 4. After initially shying away from clinical trials, she is now enrolled in one for the immunotherapeutic pembrolizumab (Keytruda).
Her treatment has been largely covered by the ACA, which was enacted in 2010 and recently survived an effort to dismantle it. The legislation was the focus of a panel held Tuesday at the American Association for Cancer Research Annual Meeting 2017.
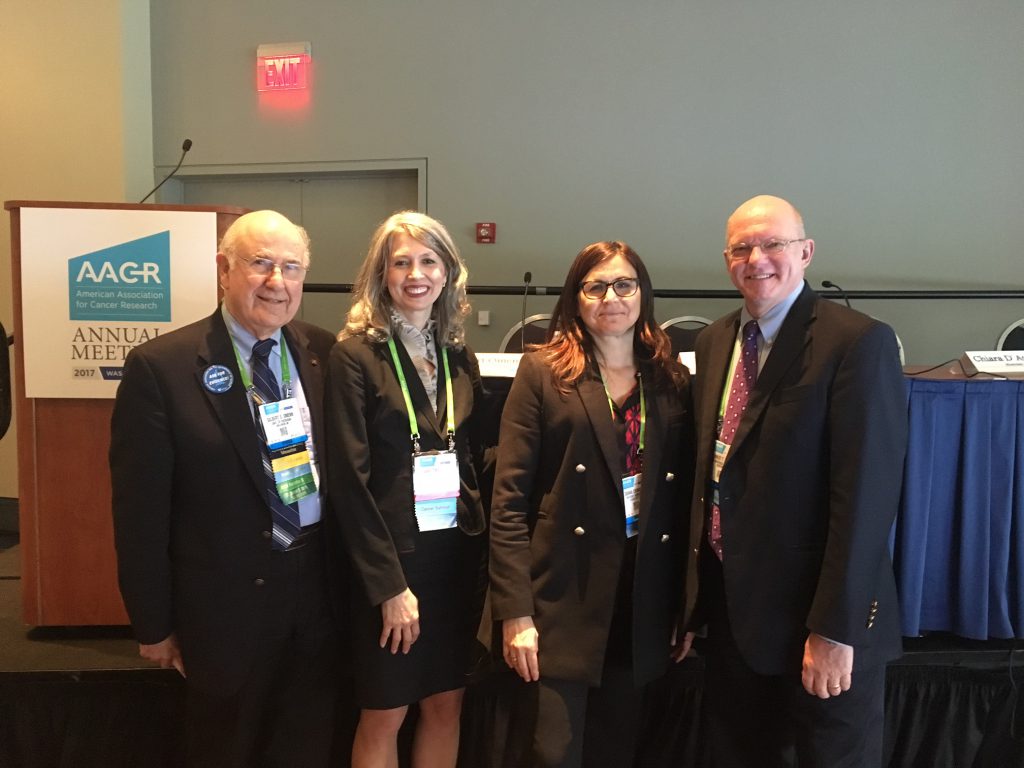
From left, Gil Omenn, MD, PhD, patient advocates Chiara D’Agostino and Diana Chingos, and Ernest Hawk, MD, MPH. The panel discussed the provisions of the Affordable Care Act that have had the most significant impact on cancer patients and survivors.
D’Agostino, fellow patient advocate Diana Chingos, and Ernest Hawk, MD, MPH, of The University of Texas MD Anderson Cancer Center, joined moderator Gil Omenn, MD, PhD, chair of the AACR Health Policy Subcommittee and a professor at the University of Michigan Medical School in Ann Arbor, for a session titled “The Key Provisions of the Affordable Care Act for Cancer Patients and Survivors.”
Omenn said cancer patients and survivors have benefited significantly from the ACA, particularly the provision that says people can’t be denied coverage due to pre-existing conditions; the prohibition of annual and lifetime coverage caps; dependent coverage up to age 26; coverage of prevention, treatment and survivorship services; and Medicaid expansion.
D’Agostino said her ACA coverage has most likely saved her life. Chingos, who battled recurrent breast cancer in the 1990s, offered a counterpoint as she explained how difficult her treatment had been as she shuffled between insurance companies and doctors, seeking providers who would accept a patient with a cancer history.
Today, she works as a patient navigator, and believes the ACA is helping patients obtain better treatment with less stress.
“Can we make the ACA better?” she asked. “Yes, we can. But not by cutting some of its lifesaving benefits.”
Hawk said the ACA has made progress in narrowing disparities in cancer incidence and mortality, due to provision of numerous measures, such as mammograms, colorectal cancer screening, and smoking cessation programs, aimed at preventing cancer or diagnosing it in early stages.
“The ACA removed an individual, personal barrier to receipt of these services,” Hawk said.
Omenn, who has advised previous administrations on health care policy, encouraged the panelists and the audience to keep speaking out about how the ACA is improving cancer treatment and prevention.
“The benefits of this law must be respected and, as far as possible, protected,” he said.