
Editors’ Picks, June 2026: Preventing Colorectal Cancer, Targeting Neural Cross-talk to Stop Glioblastoma Recurrence, and More
This June, the whole world has gathered for the most exciting event of the summer: Editors’ Picks from the journals of the American Association for Cancer Research (AACR). There may be a soccer match or two happening as well, but that’s nothing compared with the researchers who have scored big with discoveries and advances in cancer research.
The findings from this month’s highlighted studies include identifying patients with multiple myeloma who may benefit from debulking chemotherapy prior to receiving teclistamab (Tecvayli), discovering a key messenger in the cross-talk between glioblastoma cells and neurons that could be targeted to impede recurrence, assessing the potential of a shared neoantigen vaccine to prevent colorectal cancer in individuals with Lynch syndrome, and revealing considerable improvements in five-year relative survival rates of childhood and adolescent cancer patients between 1975 and 2020.
Read the full abstracts of all the featured studies below and follow the links for the full text of each article, freely available for a limited time.
Journal: Blood Cancer Discovery
Bispecific antibodies have revolutionized the treatment of multiple myeloma; however, primary treatment failure occurs in 30% to 40% of patients. In this study, we analyzed correlates of response to teclistamab and strategies to overcome primary resistance. Across two independent cohorts (n = 90), we developed the high risk of primary resistance (Hi-MM) variable, defined by extramedullary disease, plasma cell leukemia, bone marrow plasmacytosis ≥50%, or transfusion within 30 days, as a composite correlate of nonresponse. Patients without Hi-MM had overall response rates of 84% to 96% (vs. 20%–40% with Hi-MM) and significantly superior progression-free survival (P < 0.001) and overall survival (P < 0.001). Debulking chemotherapy was utilized in 19 patients; 79% then responded to teclistamab, including 100% who no longer had Hi-MM. All four patients who were primary refractory to a BCMA bispecific immediately prior to debulking then achieved deep responses to teclistamab. In conclusion, simple clinical parameters correlate with response to teclistamab, whereas debulking chemotherapy can overcome Hi-MM and successfully bridge patients to teclistamab or salvage nonresponders.
Significance: A clinically assessable composite variable, Hi-MM, identifies patients who may benefit from debulking chemotherapy prior to teclistamab. By treating patients at a time of low disease burden or using debulking chemotherapy for those with a high risk of resistance, nearly all patients can benefit from the deep and durable remissions induced by teclistamab.
Learn more about multiple myeloma:
Journal: Cancer Discovery
Glioblastoma (GBM) cells form neuron-to-glioma malignant synapses on neurite-like tumor microtubes (TM), driving infiltrative growth and recurrence. The mechanisms underlying coordinated cross-talk among GBM cells and with neurons to favor malignant over normal synapses remain largely unknown. Here, we demonstrate that glioma-secreted C1QL1 is a key messenger for glioma–neuron and glioma–glioma cross-talk to drive TM expansion and malignant synapse formation. C1QL1 binds to its receptor BAI3 on neighboring neurons and GBM cells, activating RAC1-mediated cytoskeleton rearrangement to prune normal synapses and outgrow TMs, promoting malignant synapse and glioma network formation. Targeted treatment with a non–GEF-targeting, first-in-class RAC1 inhibitor rescues C1QL1-mediated synaptic pruning, inhibiting TMs and malignant synapses to impede glioma recurrence. Our findings elucidate how cross-talk among GBM cells and neurons allows infiltrating GBM cells to sculpt and integrate into the existing neural network, highlighting a therapeutic strategy against GBM recurrence through simultaneous inhibition of TMs and glioma-induced synaptic pruning.
Significance: Our study identifies C1QL1 as a key messenger secreted by infiltrating glioma cells, orchestrating glioma–glioma and glioma–neuron cross-talk to induce TM expansion and neural synaptic pruning, driving malignant synapse formation and recurrence through a C1QL1–BAI3–RAC1 axis. Targeting RAC1 with a non–GEF-targeting RAC1 inhibitor could impede glioma recurrence and improve survival.
The article was featured on the cover of the June issue, which also included a related commentary.
Journal: Cancer Epidemiology, Biomarkers & Prevention
Background: Childhood and adolescent cancer survivors represent a growing population whose outcomes reflect both advances in therapy and late effects of treatment. We quantified trends in long-term excess mortality risk and survival using standardized mortality ratios (SMR) and relative survival, respectively.
Methods: Using the Surveillance, Epidemiology, and End Results data, we assessed 5-year relative survival and 5-year relative survival, conditional on surviving 5 years, by period of diagnosis (1975–1979 vs. 2016–2020, and 1975–1979 vs. 2011–2015, respectively). Trends were quantified by year at diagnosis using the joinpoint survival model. SMRs were estimated by 5-year time-since-diagnosis intervals and calendar-year diagnosis periods.
Results: Between 1975 and 2020, there were improvements in 5-year relative survival, with acute myeloid leukemia (AML) and non–Hodgkin lymphoma (NHL) having the greatest survival gains. For osteosarcoma, central nervous system tumors, and Wilms tumor, 5-year relative survival plateaued in recent decades. Five-year relative survival, conditional on surviving 5 years, was >90% for survivors diagnosed between 2011 and 2015 for all cancer sites analyzed. Overall, SMRs declined with increasing time since diagnosis. Excess mortality risk also decreased over calendar-year diagnosis periods, particularly during the first 5 years since diagnosis, for cancers such as lymphoid leukemia, AML, Hodgkin lymphoma, and NHL.
Conclusions: Overall, we observed considerable improvements in 5-year relative survival and declines in excess mortality risk over time.
Impact: These findings reflect advances in treatment and survivorship care. Long-term follow-up and continued research efforts are needed to understand long-term mortality risks within an evolving treatment landscape and to achieve further progress.
A related commentary was published in the June issue.
Learn about the long-term health risks experienced by survivors of pediatric cancer: Pediatric Cancer’s Aftershocks: The Challenges for Survivors Beyond Childhood
Journal: Cancer Immunology Research
Colorectal cancer remains a major global health burden and an area of urgent unmet medical need. Immunotherapy has shown limited success in colorectal cancer as most patients present with an immune-excluded, “cold” tumor microenvironment (TME). In this study, we report a dual-modality approach to treating colorectal cancer by combining the tumor necrosis factor (TNF)–based fusion protein directed to the extradomain B (EDB) of fibronectin, L19-TNF, which induces localized intratumoral inflammation and facilitates T-cell infiltration, with a CD3-based bispecific T-cell engager (TCE) targeting carcinoembryonic antigen (CEA), which mediates antigen-specific cytotoxicity. Together, these agents aim to remodel the TME, convert “cold” tumors into inflamed “hot” lesions, and broaden the therapeutic reach of immunotherapy in colorectal cancer. Immunohistochemistry confirmed coexpression of CEA and EDB across microsatellite-stable and -instable tumors. In vitro, L19-TNF in combination with a CEAxCD3 TCE significantly enhanced tumor cell killing and CD8+ T-cell proliferation. In vivo, the combination induced complete tumor regression in most animals, prolonged survival, and conferred durable protection against tumor rechallenge. Furthermore, mechanistic analyses revealed enhanced TCE extravasation, upregulated intercellular adhesion molecule 1 expression, and increased CD8+ T-cell infiltration, indicating vascular modulation and remodeling of the TME toward an inflamed “hot” phenotype. These findings confirm that targeted delivery of TNF to the TME can effectively enhance the activity of immunotherapeutic agents, such as T cell–redirecting therapies, in challenging tumor settings.
Journal: Cancer Prevention Research
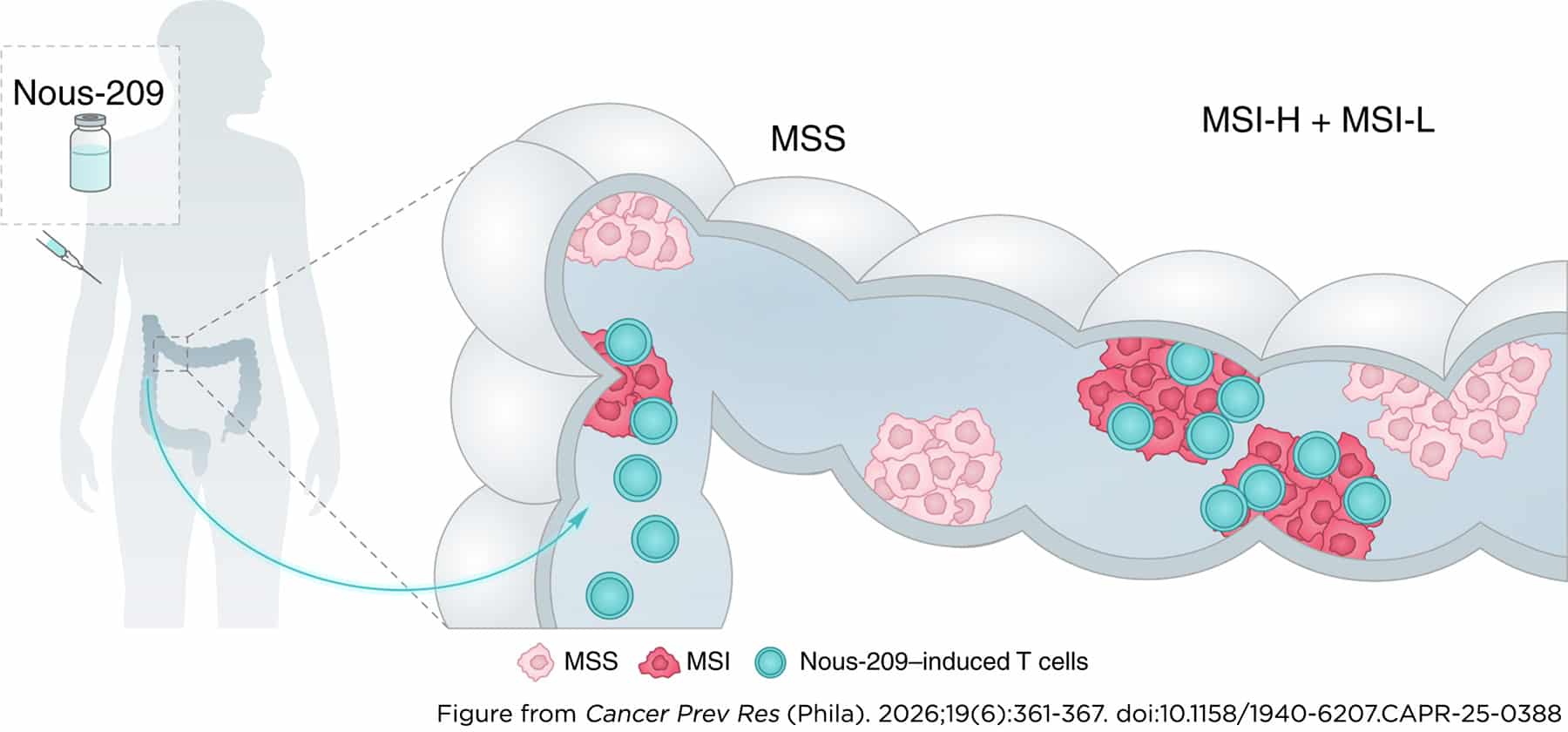
This study provides a molecular characterization of precancerous colorectal lesions in Lynch syndrome (LS) carriers to assess the preventive potential of Nous-209 immunotherapy against colorectal cancer development. A total of 50 adenomas and 12 advanced adenomas (AA) were collected from 26 LS carriers with pathogenic variants in either MLH1 or MSH2. Molecular analyses included assessment of mismatch repair (MMR) status, microsatellite instability (MSI), and detection of mutations targeted by Nous-209. We found that 83% of AAs and 58% of adenomas were MMR-deficient (dMMR). Notably, although all dMMR AA were MSI-high (MSI-H), only 66% of dMMR adenomas showed MSI-H. The presence of Nous-209 mutations correlated strongly with MSI status, with mutation counts ranging from 15 to 57 in dMMR/MSI-H lesions. dMMR adenomas classified as MSI-low carried a limited number of mutations (6–19), whereas microsatellite-stable lesions harbored very few (0–2) Nous-209 mutations, regardless of MMR proficiency. These findings confirm the molecular heterogeneity of precancerous lesions and support the potential of Nous-209 immunotherapy to prevent MSI colorectal cancer in LS by targeting the adenoma–carcinoma sequence at the time of MSI acquisition.
Prevention Relevance: Our study shows that MSI and neoantigen accumulation emerge during the evolution of precancerous lesions in LS. These findings support the clinical evaluation of Nous-209, a shared neoantigen vaccine, as an immunoprevention strategy for MSI-driven colorectal carcinogenesis, with important implications for cancer prevention research.
Learn about the clinical efficacy of Nous-209 for the prevention of colorectal cancer: Stopping Cancer Before It Starts in Lynch Syndrome
Journal: Cancer Research (June 1 Issue)
Stromal fibroblasts of the mesenchyme regulate critical signaling gradients along the crypt–villus axis in the intestine and provide a niche that supports intestinal stem cells. In this study, we reported that PDGFRA-expressing fibroblasts secrete ligands that promote a fetal-like state in the intestinal mucosa during early WNT-mediated tumorigenesis. Data from a mouse model of WNT-driven oncogenesis and single-cell RNA sequencing of mesenchymal cell populations revealed a dynamic reprogramming of PDGFRA+ fibroblasts that facilitates WNT-mediated tissue transformation. Functional assays of potential mediators of cell-to-cell communication between these fibroblasts and the oncogenic epithelium revealed that TGFβ signaling is notably induced in PDGFRA+ fibroblasts in the presence of oncogenic epithelium, and TGFβ was essential to sustain the fetal-like growth of organoids ex vivo. Reduction of CDX2 in β-catenin mutant intestinal epithelium elevated the fetal-like transcriptome and accelerated WNT-dependent oncogenic transformation in vivo. These results demonstrate that PDGFRA+ fibroblasts are activated during WNT-driven oncogenesis to promote a fetal-like state in the epithelium that precedes and facilitates tumor formation.
Significance: TGFβ signaling activated in PDGFRA+ fibroblasts in response to the initial transformation of WNT-hyperactive epithelial cells mediates expression of pro-regeneration ligands that reciprocally induce a fetal-like state in the epithelium, facilitating tumorigenesis.
Journal: Cancer Research (June 15 Issue)
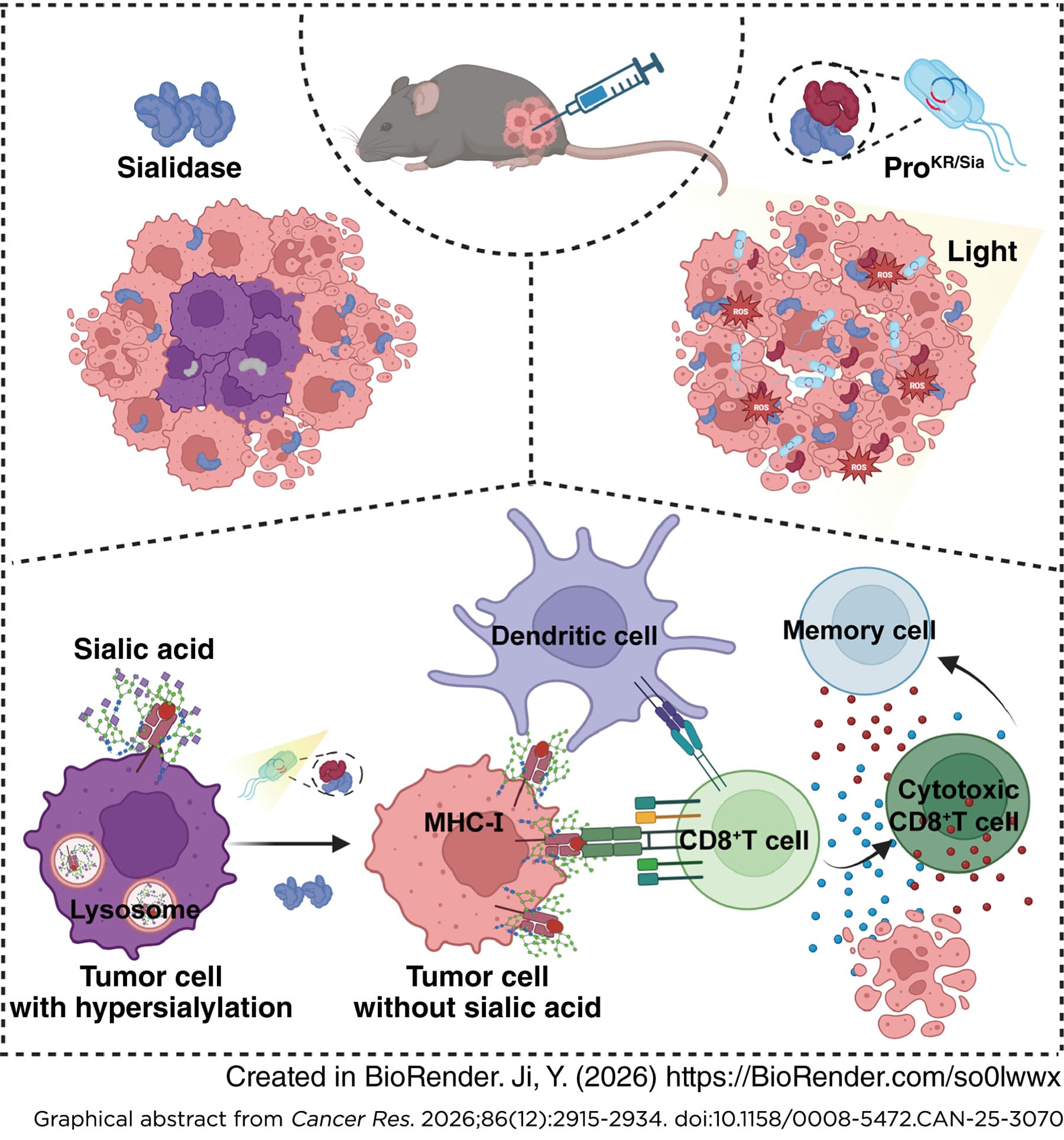
Excess terminal sialic acids on tumor glycans engage inhibitory Siglec receptors and mask peptide and glycan epitopes, including major histocompatibility complex class I (MHC-I), thereby reducing antigen visibility and dampening cytotoxic T-cell surveillance. In this study, we showed that a compact, lectin-free Salmonella typhimurium sialidase (Sia) efficiently desialylated melanoma and colorectal carcinoma cells, abolished Siglec-E binding, and spared MHC-I from lysosomal degradation. Functionally, Sia treatment enhanced dendritic cell phagocytosis and tumor antigen presentation, expanded IFNγ+/granzyme B+ CD8+ T cells, and slowed tumor growth in a CD8+ T cell–dependent manner without systemic toxicity. Engineering the probiotic Escherichia coli Nissle 1917 to coexpress the photosensitizer KillerRed (KR) and Sia (ProKR/Sia) enabled localized targeting. Following intratumoral delivery, ProKR/Sia selectively colonized hypoxic tumor cores while sparing healthy tissues; no off-target desialylation or organ colonization was detected. Brief white-light irradiation lysed the bacteria, synchronously releasing Sia to remodel tumor glycans and activating KR to generate reactive oxygen species that drive immunogenic cell death. In syngeneic murine tumor models, ProKR/Sia photodynamic therapy (PDT) outperformed either monotherapy and induced robust cellular immunity with expansion of cytotoxic CD8+ and CD4+ T cells and multiple innate responses, including natural killer cell activation and M1-like macrophage polarization. Furthermore, ProKR/Sia PDT established antigen-specific memory that rejected rechallenge. These data define a spatially confined, antigen–agnostic strategy that restores MHC-I visibility and activates antitumor immunity in immunologically “cold” tumors, leading to a durable response. Rational combinations with immunotherapy, deep-tissue illumination, and programmable biosafety switches may further overcome tumor antigen heterogeneity and broaden clinical applicability.
Significance: Probiotic sialidase-KillerRed photodynamic therapy overcomes hypersialylation-mediated immunosuppression by restoring antigen visibility and igniting durable antitumor T-cell responses, offering an antigen agnostic platform for treating solid tumors.
Learn about other efforts to target sialylated proteins in cancer: Developing Cancer Therapies at the Intersection of Chemistry and Biology
Journal: Clinical Cancer Research (June 1 Issue)
Purpose: To evaluate the efficacy and safety of pegylated liposomal doxorubicin (PLD) in the treatment of desmoid tumors (DT).
Patients and Methods: In this investigator-initiated, double-blind, phase III trial, we randomly assigned (in a 2:1 ratio) patients with advanced or refractory DTs to receive either PLD (50 mg/m2 intravenously) or placebo every 4 weeks for six cycles. Crossover from placebo to PLD was permitted upon disease progression. The primary endpoint was progression-free survival (PFS). The secondary endpoints were objective response and safety.
Results: From November 2020 to March 2023, a total of 73 patients were assigned to receive PLD (49 patients) or placebo (24 patients). With a median follow-up of 16.1 months, PLD had a significantly longer PFS over placebo (not reached vs. 4.3 months), with an HR of 0.05 (95% confidence interval, 0.01–0.17; P < 0.001). The 2-year PFS rates were 90.4% with the PLD group and 19.6% with placebo. PFS benefit favored PLD across most prespecified subgroups. The confirmed objective response was observed in 19 (40.4%) patients in the PLD group and in one (4.3%) in the placebo group (P = 0.002). Common grade 3 or higher adverse events with PLD included neutrophil count decreased (10.6%), mucositis oral (6.4%), and white cell decreased (4.3%). Significant between-group differences in certain patient-reported toxicities were observed (P < 0.05).
Conclusions: PLD significantly prolonged PFS and induced durable responses compared with placebo, with a favorable safety profile, for patients with progressive or symptomatic DTs.
A related commentary was published in the June 1 issue.
Journal: Clinical Cancer Research (June 15 Issue)
Purpose: Copy number–high (CN-H)/p53-abnormal endometrial cancers are high-grade uterine malignancies characterized by TP53 mutations, copy-number alterations, mismatch repair proficiency (MMRp), and absence of POLE mutations. A subset may be homologous recombination deficient (HRD), potentially conferring sensitivity to poly (ADP-ribose) polymerase (PARP) inhibitors. We aimed to test the combination of PARP and immune checkpoint inhibitors in this subgroup, leveraging possible synergy from immune priming.
Patients and Methods: We conducted a single-arm, open-label, phase II trial evaluating the efficacy and safety of olaparib (300 mg orally twice daily) plus pembrolizumab (200 mg intravenously every 3 weeks) in patients with persistent or recurrent CN-H/p53-abnormal endometrial cancer. Eligible patients had p53-abnormal, MMRp, and POLE-negative disease and up to 3 prior lines of therapy. The primary endpoint was the best overall response rate (ORR) at 24 weeks.
Results: Of the 25 patients evaluable for efficacy, 2 patients achieved a complete response, and 6 achieved a partial response, resulting in an ORR of 32% [90% one-sided confidence interval (CI), 19.6%–100%]. The median duration of response was 11.2 months (80% two-sided CI, 6.4–11.9). The median progression-free survival was 3.9 months (80% two-sided CI, 2.1–5.8), and the median overall survival was 16.5 months (80% two-sided CI, 9.6–23.6). No new safety signals were identified. Genomic analyses suggested that responders had a numerically higher frequency of HRD tumors than nonresponders (50% vs. 17%).
Conclusions: The combination of olaparib plus pembrolizumab has promising activity with durable responses in patients with persistent or recurrent CN-H/p53-abnormal endometrial cancer. Molecular biomarkers may be helpful for patient selection in future studies of this combination.
Journal: Molecular Cancer Research
We generated 64 epigenomic datasets using chromatin immunoprecipitation with sequencing and assay for transposase-accessible chromatin sequencing profiling on 28 fresh bladder cancer specimens of luminal and basal-squamous expression subtypes. An integrated analysis of core regulatory circuitry, enhancer activity, and transcription factor (TF) expression specificity nominated 23 luminal-specific and 14 basal-squamous–specific candidate master TFs (MTF), including established regulators like FOXA1, PPARG, and GATA3 for luminal bladder cancer and TP63 for basal-squamous bladder cancer, as well as new basal-squamous MTF candidates, SNAI2 and CEBPB. GRHL2, a regulator of subtype differentiation, was identified as a common MTF to luminal and basal-squamous bladder cancers. Cis-regulatory elements were enriched up to 80-fold for bladder cancer risk variants. Keratinization pathways were enriched in genetically determined basal-squamous sites, whereas carcinogen glucuronidation pathways were enriched in luminal sites. Integrating germline variation and epigenomics through a cistrome-wide association study identified a new bladder cancer risk locus upstream of SPINK1 and linked 10 of 19 bladder cancer risk loci to regulatory elements from a 350,000-sample genome-wide association study.
Implications: Overall, this integrative computational analysis provides comprehensive insights into the epigenomic underpinnings of bladder cancer subtypes, nominates candidate master regulators of cellular identity for future experimental validation, and reveals how regulatory elements harboring inherited germline variation may contribute to bladder cancer risk and biology.
Journal: Molecular Cancer Therapeutics
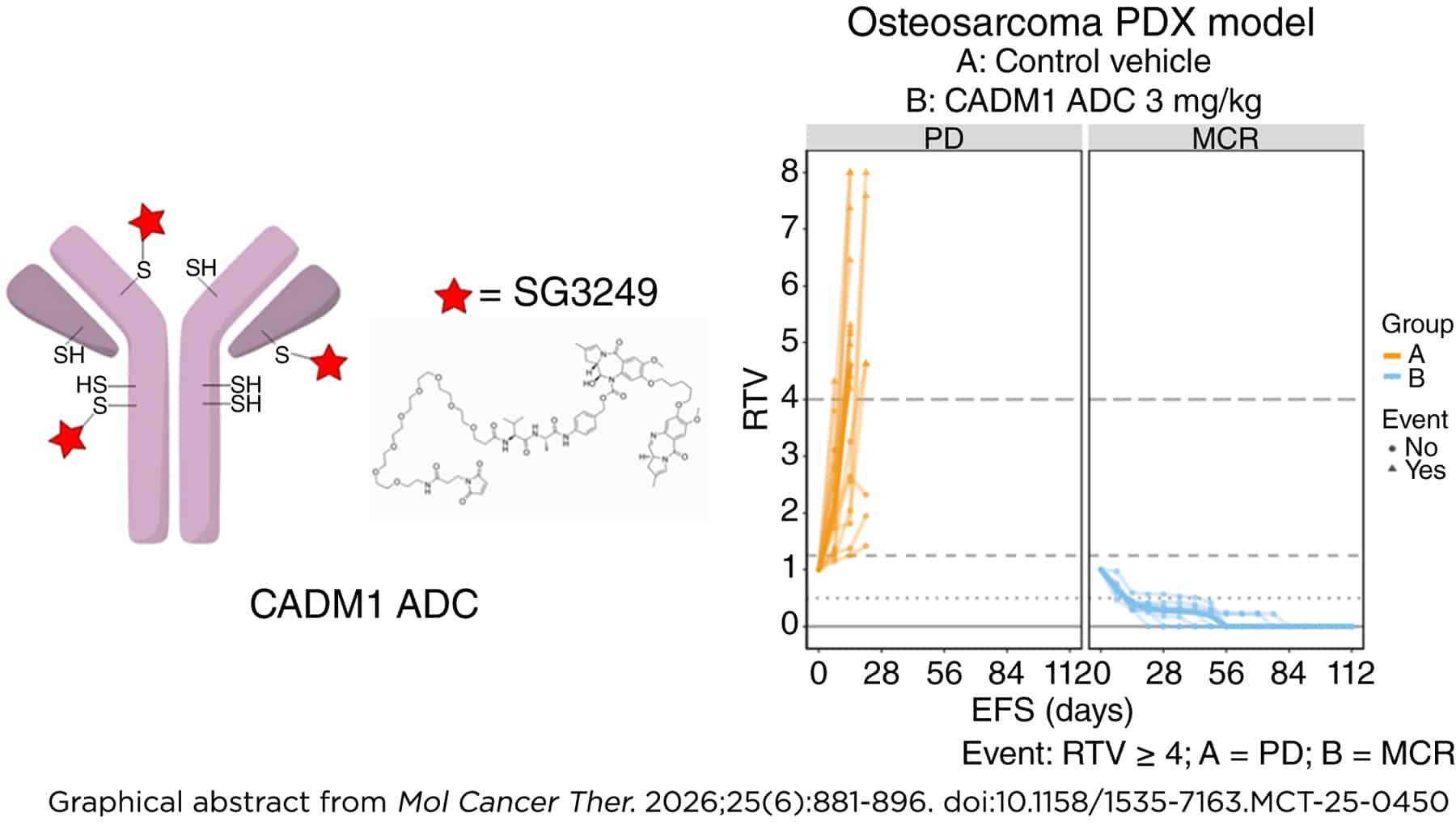
Due to the paucity of validated cell-surface osteosarcoma-specific targets, patients with this condition have long been excluded from the benefits of antibody–drug conjugate (ADC) therapy observed in patients with several solid and hematologic malignancies. Our comprehensive surfaceome profiling approach previously identified osteosarcoma-specific cell-surface antigens that are highly expressed in osteosarcomas but minimally expressed in normal tissues. As a result, one such antigen, CADM1, was selected for the generation of an ADC. We tested a CADM1-targeting ADC with a tesirine payload (SG3249) in vitro in osteosarcoma, rhabdomyosarcoma, and neuroblastoma patient-derived xenograft (PDX) cell lines. In vivo, we tested six CADM1-expressing osteosarcoma PDX models. The CADM1 ADC demonstrated significant antitumor activity in vitro across the osteosarcoma, rhabdomyosarcoma, and neuroblastoma cell lines. Additionally, it effectively reduced tumor volume and extended event-free survival in all six osteosarcoma PDX models tested. Notably, the CADM1 ADC achieved a major complete response in one model (OS2), complete responses in two models (OS1 and OS33), and partial responses in three models (OS9, OS17, and OS31). Based on these results, clinical development of CADM1-targeted therapies for osteosarcoma and other CADM1-expressing pediatric solid tumors may be warranted.
Journal: Cancer Research Communications
One strategy for enhancing the anticancer immune response is to inject tumors with immunostimulatory agents that modify the tumor microenvironment (TME) to induce a stronger antitumor T-cell response. In situ immunization with vidutolimod (Vidu), a virus-like particle containing a CpG-A TLR9 agonist, has demonstrated antitumor activity in preclinical and early-phase clinical studies; however its effect on tumor-specific CD8+ T cells remain poorly defined. Using the OT-1 model, we assessed how Vidu affects the activation, cytotoxicity, and antitumor activity of tumor-specific CD8+ T cells in vitro and in vivo. In vitro, Vidu reduced proliferation but increased expression of both activation and exhaustion markers. In vivo, repeated intratumoral Vidu injections induced a transient increase in the frequency of intratumoral tumor-specific CD8+ T cells and enhanced antitumor activity. The addition of αPD-1 to Vidu led to a persistent increase in intratumoral tumor-specific CD8+ T cells and sustained tumor control. Vidu treatment increased expression of markers associated with terminal exhaustion on intratumoral tumor-specific CD8+ T cells. Such treatment also increased the number of circulating tumor-specific CD8+ T cells that expressed high PD-1 but lacked coexpression of other exhaustion markers. Together, these findings demonstrate that Vidu treatment expands the number of intratumoral and circulating tumor-specific CD8+ T cells and that the number of tumor-specific CD8+ T cells and the antitumor response is sustained by the addition of αPD-1. These results support continued evaluation of Vidu as a cancer immunotherapeutic agent, including in combination with immune checkpoint blockade.
Significance: In situ immunization with Vidu combined with αPD-1 therapy enhances the antitumor response by tumor-specific CD8+ T cells by expanding the systemic and intratumoral populations. These findings demonstrate how Vidu alters T-cell biology and supports its continued development, particularly in combination with checkpoint blockade to optimize antitumor immunity.


